




Introduction
Acute lymphoblastic leukemia (ALL) is one of the few cancers that impact the entire lifespan, from the neonatal period to the very elderly. Although survival rates now approach 90% for most children with ALL, older adolescents and young adults (AYAs) historically have poorer prognosis, with an event-free survival (EFS) of 30 to 45%.1–8 The past decade has witnessed a dramatic advancement in the management of AYAs with ALL. The application of pediatric ALL protocols by medical oncologists, the understanding of the molecular basis of ALL, the incorporation of sensitive measures of MRD, and new therapeutic agents are changing the landscape of ALL for this population.8,9
The therapeutic progress achieved with pediatric regimens in childhood ALL has contributed to the increase of their use in the AYA population worldwide, in an attempt to achieve a better survival. The outcome of AYA’s with ALL has not been published in Lebanon, neither has the therapy related complications, morbidity and mortality rate. Hence, we decided to conduct a retrospective chart review to include all adolescents aged 12-18 years old, diagnosed with ALL, treated at Children’s Cancer Center of Lebanon, based on the “CCCL/ALL I Study for newly diagnosed patients with Acute Lymphoblastic Leukemia”, enrolled since October 2011 until March 2019.
Materials and methods
Between October 2011 and March 2019, a total of 38 patients, aged between 12 and 19 years old, were diagnosed with Acute Lymphoblastic Leukemia at the Children’s Cancer Center of Lebanon, and they were enrolled in the CCCL/ALL I Study for newly diagnosed patients with Acute Lymphoblastic Leukemia, that’s based on the SJCRH total XV protocol.
Data collected included sex, age at diagnosis, initial WBC count, ALL immunophenotype, extramedullary disease (if present), flow cytometry results, bone marrow karyotype, leukemia molecular genetics, DNA index, minimal residual disease (MRD) by flow cytometry and molecular analysis whenever available, on days 15, 22, end of induction, and any additional date, if performed; risk stratification, need for re-intensification, total number of intrathecal chemotherapy, missed/interrupted chemotherapy, dose reduction, complications, relapse and mortality.
The diagnosis of ALL was based on the presence of leukemic blasts on flow cytometry on bone marrow exam or on peripheral blood when the bone marrow wasn’t done.
Therapy was given according to the SJCRH total XV protocol. The total XV protocol stratified patients into low, intermediate and high risk based on the patient’s clinical data as well as the blast’s immunophenotype and genotype. The main aims of this study were to estimate the EFS of children aged more than 1 years diagnosed with ALL and treated with risk directed therapy, and the implementation of MRD at the end of induction to further stratify patients; the safety of omission of CNS irradiation and assessing the prognostic value of biologic markers in childhood ALL. The treatment details are summarized in table 1.
IBM SPSS 26.0 was used to analyze the data. The results are presented below, and the level of statistical significance was set at p value <0.05
Results
Patients and their response to treatment
Since October 2011 until March 2019, a total of 38 patients aged between 12 and 18 years of age were diagnosed with Acute Lymphoblastic Leukemia and were treated according to the CCCL/ALL I Study for newly diagnosed patients with Acute Lymphoblastic Leukemia, based on the SJCRH total XV protocol.
The median age at diagnosis for both males and females was 15 years old. 66% of patients were males, where the median age at diagnosis was 15 years; 34% of the patients were females, with the median age at diagnosis being 13.5 years. Of those patients, 79% had B lineage ALL, 13% had T lineage ALL and 8% had mixed/biphenotypic ALL.
10% had Philadelphia chromosome positive B cell ALL, with 75% being females; those patients were treated according to the high risk protocol; 2 of those patients received stem cell transplantation, the first proceeded to transplant upfront, after intensification chemotherapy, while the other proceeded to transplant upon early isolated bone marrow relapse.
Only 1 patient had TEL-AML1 translocation t(12;21), and was treated according to the low risk group. 13% (n=5) of the patients had hyperdiploidy, with DNA index >1.16, 4 of those were treated as per the LR protocol, while the other patient was upgraded to the SR protocol due to positive bone marrow exam by flow cytometry at day 15 of induction.
42% of the patients had an MRD <1% at induction day 15, and 92% of patients had a negative bone marrow exam with MRD <0.01% at the end of induction. 1 patient passed away during induction chemotherapy at day 40, secondary to sepsis leading to multiple organ dysfunction syndrome and death.
31% of our patients had an abnormal karyotype upon presentation. And 2 of the patients who had an initial normal karyotype, relapsed with an abnormal one. By using chi-square test, there was no statistical significance between the presence of an abnormal karyotype at diagnosis or upon relapse and the dismal outcome in terms of relapse or mortality.
Complications: graded as per the CTCAE-2017
Complications were classified into infectious and non-infectious. To begin with, significant treatment related infections, leading to either major delays in chemotherapy (where 2 or more weeks of treatment interruption occurred) or major omission of treatments (more than 10% of the total duration of treatment) or significant morbidities and mortalities, occurred in 34% of patients. Infectious complications are summarized in table 2.
The major non-infectious complications occurred as follows: Thrombosis: 25% experienced thrombosis, most commonly sagittal venous thrombosis, mainly occurring during the first 20 weeks of maintenance chemotherapy (n=9), where the majority experienced grade 2 thrombosis, requiring medical intervention (LMWH), whereas one patient had extensive left pulmonary embolus (the same patient who experienced severe infection and multiorgan failure during induction, leading to death). Interestingly, 42% (n=14) of our patients had AVN, and that percentage doubles the incidence that has been reported in literature, albeit it is known that adolescents have the highest incidence of AVN among the other age groups, when treated for ALL. Where 30% of those patients had a grade 3 AVN, requiring elective hip replacement whether unilateral or bilateral, and the remaining 70% were having grade 2 AVN. The incidence of pancreatitis was 36% (n=13), where 15% of those (n=2) had grade 3 pancreatitis, with one patient developing pancreatic hemorrhage, necrosis and pseudocyst formation, requiring transfusion, parenteral feeding and later intervention and another patient required major modification in his chemotherapy, where he missed asparaginase since week 7 of maintenance, and ended up relapsing and requiring stem cell transplantation.
Mortality occurred in 5 patients (14%), with one patient dying during induction, one patient dying after bone marrow transplantation after an early isolated medullary relapse, the third patient suffered from multiple relapses, and passed away upon relapsing after a second bone marrow transplantation, the fourth patient passed away secondary to septicemia during reinduction chemotherapy, and the last patient suffered from multiple relapses and passed away after CAR – T cell therapy.
Chi-square test was used to estimate the effect complications on the patient’s outcome (relapse and mortality). Tables 4 & 5 shows the chi-square test results for mortality and relapse rate respectively:

Event Free Survival and Overall Survival
IBM SPSS 26.0 was used to analyze the data. The results are presented below, and the level of statistical significance was set at p value <0.05. EFS over a 5 years’ period since diagnosis was 80%, whereas overall survival was 86%.
The estimated 5-year OS and EFS by gender (Figure 1,2), showed that there was no statistically significant difference between male and female cases, (p=0.366 and p=0.252, respectively).


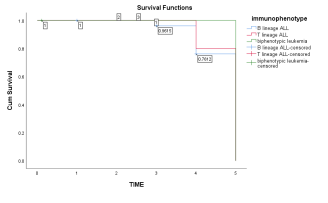
By analyzing survival data in terms of the leukemia’s immunophenotype (Figures 3, 4), there was no statistical significance in terms of 5-year estimated OS and EFS (p=0.738 and p=0.718, respectively).


The survival in terms of risk stratification (Figures 5, 6) showed that there was no statistical significance between cases in terms of 5-year estimated OS and EFS (p=0.262 and p=0.373, respectively).


Discussion
Treatment of ALL involves some of the most complex chemotherapy regimens and treatment schedules used in oncology. First, induction chemotherapy is used to reduce the burden of lymphoblasts in the bone marrow and to restore normal hematopoietic function. Second, consolidation therapy is used with the intention of clearing any drug-resistant leukemia cells that have survived induction therapy and to eliminate minimal residual disease (MRD). Third, maintenance chemotherapy consists of 2 to 3 years of low-dose antineoplastic drugs designed to prevent leukemia relapse during the crucial few years after remission induction and consolidation. Finally, central nervous system (CNS) prophylaxis is necessary to treat/prevent CNS leukemia as the CNS is shielded from systemic therapy by the blood-brain barrier.5,8,10,11
In general, pediatric trials for ALL treatment consist of higher cumulative doses of non myelosuppressive agents (glucocorticoids, Vincristine and Asparaginase), with early initiation of CNS prophylaxis, during induction chemotherapy, continuing throughout maintenance chemotherapy, thus achieving a higher cumulative dose of intrathecal chemotherapy than adult protocols, and continuing long-term maintenance for a longer period, particularly for male patients. Whereas the adult trials often focus on dose intensification of the myelosuppressive agents, including cyclophosphamide and anthracyclines.2,4,6,10,12,13
Our data for AYA’s treated as per the pediatric ALL protocol aged between 12 and 18 years at diagnosis showed a similar EFS and OS in comparison to the data published internationally, where the EFS was 80% and the overall survival reached 86%. The French, Dutch, UK, and US comparisons all demonstrated significantly higher survival rates when teenagers (13- 21 years old) were enrolled on pediatric rather than adult trials. The Dana-Farber Cancer Institute published their own results in subsets of teenaged patients treated on 2 consecutive trials, the 5-year EFS and OS rates for patients aged 15 to 18 years on those trials were 77.5% and 81%, respectively, which was comparable to the results reported in the younger, lower risk group of patients aged 10 to 15 years. St. Jude’s Children’s Research Hospital achieved a 5-year EFS and OS rates at 86.4% and 87.9%, respectively, for patients aged 15 to 18 years, where investigators used an MRD-directed treatment in a cohort of 45 patients treated in Total Therapy XV.1,2,14–16 Similarly, retrospective data from the MD Anderson Cancer Center using the HYPER-CVAD regimen have also reported favorable results in their AYA patients. With a median age of 19 years, the CR rate was 97% for 102 AYAs with newly diagnosed ALL and OS was 65%.17
An exception occurred in Finland, where the adult trial adhered more closely to the pediatric treatment regimen, and no significant differences between adult and pediatric therapy were detected. In this study, a group of 128 patients aged 10 to 16 years treated on pediatric protocols were compared with 97 patients aged 17 to 25 years. There was no significant difference in the 5-year EFS (67% for the pediatric group and 60% for the adult group) or OS (77% in the pediatric group and 70% for the adult group). Interestingly, in this comparison, there were no significant differences in the doses of corticosteroids,vincristine, or asparaginase between the pediatric and adult trials, although the pediatric trials contained higher cumulative doses of methotrexate and, in the adult protocols, more anthracycline.18
In terms of disease characteristics, including high-risk features, our data again showed similar results to those published internationally. For instance, the incidence of T cell ALL in our population reached 13%, in addition, Philadelphia positive ALL was found in 10%, also, an abnormal bone marrow karyotype was detected in 31% of the patients. In comparison, potentially better outcome features including TEL-AML 1 translocation occurred in 2.6% only. In the data published by the University of Texas MD Anderson Cancer Center (MDACC) in Houston, the presence of trisomies of chromosomes 4, 10, or 17 in the AYA population was rare, and the percentage of patients with T-cell phenotype and with the BCR-ABL-like molecular signature were higher in the AYA population. Also, only 2.6% of our AYA patients had an extramedullary disease upon presentation which is lower than the internationally reported incidence (8-12%).
In terms of therapy related morbidities, our data showed a similar rate of thrombosis and pancreatitis as well as delay in chemotherapy administration in comparison to international data. For example, thrombosis occurred in 25% of our AYA patients receiving asparaginase, which is similar to the internationally published data. according to age is one of the main issues with asparaginase. Severe acute pancreatitis occurred in 9% of our patients with international data rates varying from 2.3% to 7% in large cohorts.3,16,19
Interestingly, our data showed a higher incidence of avascular necrosis, reaching 42%, and that occurred in 14 patients aged between 12 and 17 years of age, with a median age of 14.7 years. The avascular osteonecrosis incidence in the NOPHO 2008 study was 1.5% for patients age 1 to 9 years, 13.4% for those age 10 to 17 years, and 8.5% for those aged more than 18 years. The only proven intervention for prevention has been the successful split of dexamethasone during delayed intensification proposed by the Children’s Oncology Group. AVN tends to be multifocal and occurred within the first 2 years since diagnosis of ALL in young adults. And the incidence of AVN was highest among this age group, reaching 15% in patients aged less than 20 years old, in comparison to 3% in patients aged more than 20 years.20,21
As mentioned, most of our results resembled the international results in terms of patient’s characteristics- apart from a narrower age range (up to 18 years in comparison to other results where ages up to 39 years were included), disease characteristics and outcomes, though our population tended to have a higher incidence of AVN. Limitations in our study included the small number of patients, lack of reporting of iAMP 21 at diagnosis, which would have led to better understanding of the disease, better risk stratification and perhaps better outcome of patients.
Conclusion
Progress in the field of treatment of Acute Lymphoblastic Leukemia in adolescents and young adults has been dramatic over the past few years, through the identification of new genetic entities and the adoption of fully pediatric or pediatric-inspired protocols. Risk stratification based on recent biological findings and sequential MRD evaluations should now be implemented, as should new therapeutic options including immunotherapy and targeted therapies, preferably within the setting of integrated pediatric protocols. Our data, at Lebanon, at the Children’s Cancer Center of Lebanon, was comparable, in terms of survival, to similarly aged patients treated with other pediatric ALL protocols, worldwide. The complication rate was similar as well, though our patients tended to have a higher incidence of avascular necrosis, almost doubling the incidence of AVN in published outcomes of similarly aged patients. This necessitates further research in the genetics field to try justifying this increased tendency of AVN upon treatment of ALL in adolescents and young adults in Lebanon, as well as further research on minimizing the effect of treatment in this age group. In addition, further implementation of the leukemia molecular genetics need to be done, so that higher risk patients can be identified upfront and their treatment approach tailored appropriately, aiming for a higher cure rate.
Conflict of Interest
None
Funding Information
N/A
Ethical Statements
The study was initiated after an IRB approval was granted from the American University of Beirut- research center.
Acknowledgement
Lara Ghaddar, MD; all the staff at Children’s Cancer Center, American University of Beirut Medical Center.
Author Contributions
I. conception and design: All authors
II. data collection and assembly: All authors
III. data analysis, manuscript writing: All authors
All authors have approved this manuscript.