Introduction
Vancomycin is a critical antibiotic utilized in the management of severe bacterial infections, especially Staphylococcus aureus, among pediatric patients with various oncological diseases. Accurate dosing of vancomycin is crucial to ensure therapeutic success and minimize the risk of treatment failure. However, under-dosing of this antibiotic can lead to suboptimal drug levels, which may compromise its efficacy.
Therapeutic drug monitoring (TDM) and pharmacokinetic modeling have emerged as valuable tools in pediatric medicine, aiding in the optimization of drug dosing regimens. By monitoring drug concentrations in the blood and utilizing pharmacokinetic models tailored to the specific patient population, healthcare professionals can individualize treatment plans and make informed dose adjustments.1
In 2017, Pakistan has reported 40480 deaths, in children under 5 years of age due to lower respiratory infections.2 In a study by Shahid et. al. it was reported that Staphylococcus aureus carriage prevalence was 5.6% (n=176), and 50.1% (n=81) of the isolates were methicillin-resistant Staphylococcus aureu (MRSA).3 In a study Sadia et. al. 14.% children (n=346) showed growth of MRSA in nasal samples.4
While therapeutic drug monitoring of vancomycin has been applied in pediatrics, the evidence base and practical recommendations for its use remain moderately established. Therefore, there is a need to further explore and identify knowledge gaps in this area, directing research efforts towards refining vancomycin dosing strategies specifically in pediatric patients.
The objective of this study was to assess the incidence of achieving steady-state trough concentrations in pediatric patients with complicated infections and oncological diseases, using a vancomycin dosing regimen of 15 mg/kg per dose administered every 6 hours. Additionally, the study aimed to evaluate the necessity and safety of dose adjustments based on therapeutic drug monitoring results.5
By investigating the efficacy and safety of this standard dosing regimen, the study aimed to shed light on potential improvements that can be made to optimize vancomycin therapy in this vulnerable population. The findings from this research can inform healthcare professionals and researchers about the need for dose adjustments, increased dosing, or altered dosing frequency to achieve target trough concentrations of vancomycin.
The present article summarizes the study’s methodology, patient characteristics, and key results, highlighting the implications for clinical practice and the need for further investigation to refine vancomycin dosing strategies in pediatric patients with complicated infections and oncological diseases.
MATERIALS AND METHODS
Materials
The blood sample was collected by a staff nurse and sent to the pathology lab at Shaukat Khanum Memorial Cancer Hospital and Research Center for the evaluation of vancomycin levels, serum creatinine, blood urea nitrogen, and other tests to calculate the creatinine clearance to check kidney performance and vancomycin levels.
Ethical Approval
Current study was approved by REC-Riphah Institute of Pharmaceutical Sciences (RIPS) Approval Board for Human/Animal Studies with IRB reference number REC/RIPS-LHR/2023/721.
Data collection
Study Center
This retrospective study was conducted at Shaukat Khanum Memorial Cancer Hospital and Research Center, Lahore, Pakistan from November 2022 to April 2023.
Methods
Study Population
The study population consisted of 100 male and female patients with different infections who are previously diagnosed with oncological infections. The study population comprised sixty (60) male and forty (40) female pediatric patients with an age range of 3 months to 15 years.
Inclusion Criteria
-
The data were evaluated in patients aged 3 months to 15 years.
-
Those patients, whose samples were drawn appropriately, as per instructions and guidelines provided by the institution, at steady-state level (before half an hour of the fourth or successive dose).
-
The patients who received more than one course of VCM, during the duration of the study, only the initial course was considered and added to the study for analysis.
-
The patients, who received only 24-48 hours of vancomycin therapy, despite the failure of attainment of required trough concentrations, were included.
-
Collected data, comprised of demographic features, VCM doses, intervals for administration, the particular serum trough levels, blood urea nitrogen, and serum creatinine levels.
Exclusion criteria
-
Patients who have a history of hypersensitivity or allergic reactions to vancomycin
-
Patients with known or suspected renal impairment (such as renal failure, creatinine clearance <30 ml/min/1.73m²) or those on dialysis
-
Patients who have received concomitant treatment with other nephrotoxic drugs or those who have taken non-steroidal anti-inflammatory drugs (NSAIDs)
-
Patients who have received vancomycin for prophylactic or surgical purposes
-
Patients with incomplete or missing data on demographic information, VCM doses, intervals for administration, inappropriate serum trough levels drawn, and serum-creatinine levels.
Study Design
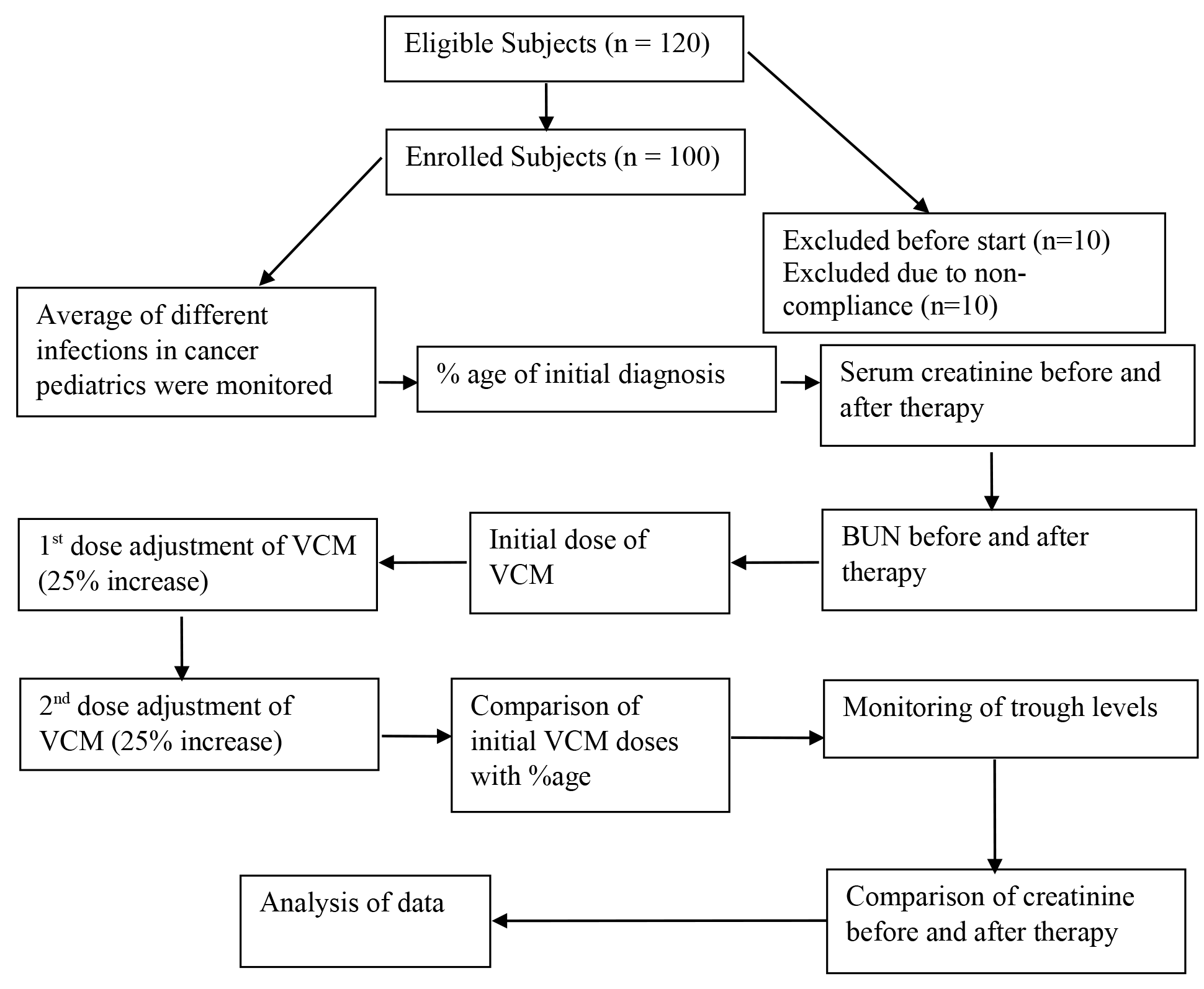
A cross-sectional retrospective analysis was conducted, and drug concentrations were monitored in all children receiving VCM. Dose adjustments were performed in case of lower or higher drug concentrations as compared to standards. Trough concentration levels were obtained by taking the samples 30 minutes before infusing the fourth VCM dose. Serum creatinine levels were also monitored as a parameter to check nephrotoxicity. Data of children with VCM trough concentrations were collected. Data including age, weight, serum creatinine, VCM dosage, and VCM trough concentrations were collected.
Significance
VCM is administered to patients, suffering from serious and fatal infections, caused by gram-positive bacteria, which are resistant to other less potent agents. The standard range of concentration for the VCM trough levels is in the range of 10 to 20µg/ml. Whereas, the reference concentration range for VCM peak levels is 25 to 50µg/ml. In pediatric patients due to high creatinine clearance, the plasma levels of the drug are not achieved. So dose adjustment has significance to achieve the trough level, especially in pediatric patients with cancer and having high creatinine clearance. In this study, a P-value of < 0.05 was taken as significant
Statistical Analysis
Statistics were applied by using Graph Pad-Prism ver. 8.4.3. Categorical variables like weight have been reported as frequencies and percentages. Unpaired t-test and Analysis of variance ANOVA (one-way ANOVA)was employed, followed by posthoc for the comparison of the efficacies in all treatment groups and significance (P-value < 0.05) of the observed outcomes of the study. The final data representation comprises bar graphs, tables, and flow charts.

RESULTS
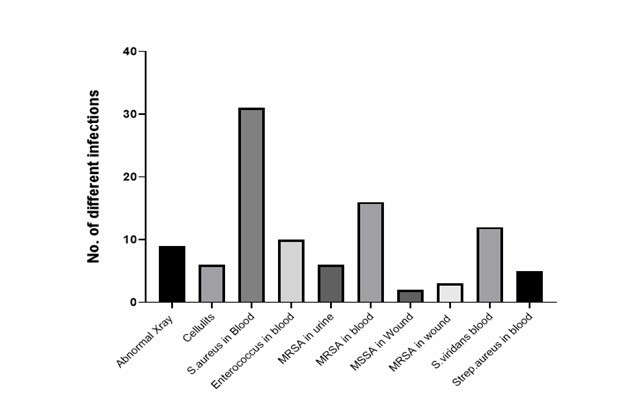
The frequency of pediatric cancer patients with oncological infections at Shaukat-Khanum Memorial-Cancer Hospital and Research Center is as shown in Figure 1 with the cause of infections that required the treatment with antibacterial agents of a broader spectrum like VCM to reduce the risk of disease and death, associated with the infections. For strains of MRSA, with minimum inhibitory concentrations above 2μg/ml, VCM is considered to be ineffective; because its serum-protein binding raised up to 50%. Therefore, trough concentration levels of VCM must be 15-20μg/ml for effective eradication of invading strains with a MIC of 2μg/ml.

The different types of cancer that occur most commonly in male and female pediatrics at Shaukat Khanum Memorial Cancer Hospital and Research Center are shown in (Supplementary Figure 1 & Figure 2) in which VCM was used for different bacterial infections as discussed above. The Pre B cell acute lymphoblastic leukemia (Pre B ALL) frequency was higher in comparison with Wilm’s Tumor and other types of cancer in male and female pediatrics such as Burkitt’s, Osteosarcoma, Ewing’s Sarcoma, Diffuse Large B-cell Lymphoma (DLBCL), and many others. Pre-B ALL patients carry more infections due to low neutrophil counts as compared with other cancers and need a long duration of therapy with VCM.
The TDM of VCM in pediatrics targets a trough concentration of 15–20 mg/L for appropriate therapeutic effectiveness. A comparison of initial and final doses used with a 25 % increase in VCM doses is shown in (Supplementary Figure 3). Due to higher creatinine clearance in pediatrics, the dosage of the VCM needed adjustments. Initially, a 25% increase depending upon the infection and creatinine clearance rate showed (p= 0.0001) significant outcomes. Initial dosing vs 1st dose adjustment showed less significance (p= 0.0332). Initial dosing vs percentage increase 2nd dose showed significant outcomes (p= 0.0001), while 1st dose adjustment vs 2nd dose adjustment showed insignificant outcomes (p=0.9322).
Supplementary Figure 4 demonstrates the difference between the mean minimum and after-treatment, creatinine level with SEM values (0.057 ± 0.042) and (p = 0. 6296), hence showing insignificant outcomes.
Creatinine and BUN levels were the mainstays of measuring the renal function of the patients before and after the completion of VCM therapy. The comparison in BUN values before and after the therapy is shown in (Supplementary Figure 5). The comparison between minimum BUN vs. BUN after dosing remains comparatively less significant (P = 0.0407) and SEM values (2.890 ± 0.5398) but with the provision of normal levels that not affecting the overall health of the patients.
Discussion
The are certain dose consideration for VCM maintenance dosing, these include predialysis trough level, patient weight, and period to the next dialysis session in the pediatric patients undergoing hemodialysisic. The loading dosage can be high cover serum levels for the period to the next scheduled dialysis in comparison to fixed loading doses used.6 Generally, dosage is 15 mg per kg per dose which is given after interval of every 6 hours, compared to a 10 mg per kg per dose every 6 hours, is more likely to achieve target trough concentrations of 15–20 mg/L and the goal AUC/MIC ≥ 400 mg per liter per hour.6 The recent dosing guidelines refer to the basic pharmacokinetics and pharmacodynamics of VCM as well as reports from clinical studies. Expert analysis is targeting on provision of evidence of superiority of administering vancomycin by continuous infusion compared to intermittent infusion; this evidence focuses on revising the current practice of specifically trough monitoring in comparison to the AUC–time curve and evaluation of weight-based dosing versus AUC-based dosing7 Such practice has not been practice in participants healthcare settings, but shall require due diligence, as current practice has produce safety and efficacy.
In current study Staphylococcus aureus was reported the highest in blood stream infections. In a study by Cook et. al. in pediatric patients seen for bloodstream infections, the gram positive infections were 44.8% and Staphylococcus aureus was the most common isolate with 19.3% prevalence.8 In present study Pre B ALL was the most common cancer diagnosed in both female and male patients. In a 11 year study at a tertiary hospital the most common cancer among the pediatric patient was soft tissue and bone sarcomas 23.2%.9 The variation can be attributed to higher incidence of neutropenias leading to infection in Pre B ALL patients. However, current study depicted the dose adjustment of vancomycin commonly at 22.5 mg per kg per dose, another study at a tertiary care hospital, found significant improvement in optimal doses adjustment 50.6% without pharmacist involvement and 88.8% when dosing is directed by pharmacist.10 In present study after the treatment of susceptible infections with VCM, the serum creatinine and blood urea nitrogen remained within the normal ranges, provision of normal levels that not affecting the overall health of the patients. In study by Hirai et. al. 17.3% patients had developed VCM nephrotoxicity whereas VCM trough levels improved to 10–20 μg/mL among 75% of the study patients.11
Various pharmacokinetic models have been generated for VCM, however external validation of recommended dosing regimens and analyses in subgroup pediatric populations such as dialysis patients are still needed before. Application of such model with patient to patient variations, which is dependable on essential therapeutic drug monitoring.12 VCM pharmacokinetics are characterized by fat-free mass, serum creatinine, blood urea nitrogen, dialysate flow rate, and ultrafiltration rate in the pediatric dialysis population. Dosing of 40–50 mg per kg per day on fat-free mass divided every 8–12 hour with frequent vancomycin serum sampling is recommended.13 Augmented renal clearance is frequently observed in pediatric patients with post-transplant febrile neutropenia, resulting in a significant increase in VCM clearance. Likewise, rapid clearance can be observed in the present study, with better results after 2nd dose adjustment. Although Shitmamoto et. al. suggests VCM in neutropenic patients based on glomerular filtration rate, age, weight and body temperature.14 Moffet el. al. suggests appropriation of VCM dosing based on pediatric patients weighing ≥70 kg (weight based versus non-weight based) to achieve an AUC-time curve ≥400 mg per liter per hour and a trough concentration of <20 mg per liter. Current study also utilized weight based dosing using fat-free mass, with active dosage adjustment of VCM for renal impairment dependent on pediatric population pharmacokinetic analysis.13
Present study saw no significance in serum creatinine and BUN, whereas, Totapally et. al. Reported that critically ill pediatric patients, the acute kidney injury is reversible during VCM therapy is associated with an elevated BUN: Serum creatinine ratio.15 According to Williams et. al. study which included a cohort of 12,730 children with reported incidence of VCM induced acute kidney injury in 11.8%. children.16 The median age of the cohort was 2.5 years, and 57% of the patients were male. The risk factors for VCM induced acute kidney injury were the concomitant use of nephrotoxic medications, increased trough concentrations, longer duration of treatment, impaired renal function, and the need for pediatric intensive care.16
Conclusion
This study indicates that patients who require trough concentrations of 15-20 micrograms/ml may struggle to attain the desired therapeutic levels using the current dosing regimen of 15 mg/kg every six hours. Therefore, dose adjustments may be necessary to achieve the desired therapeutic drug levels. However, it is important to initially administer doses within the range of 15-20 mg/kg every six hours, as vancomycin can have nephrotoxic and ototoxic effects at trough concentrations higher than 20 micrograms/ml. Based on the study’s findings, it is recommended to utilize a higher initial dose of vancomycin to achieve target trough levels early on and improve therapeutic outcomes. However, further research is necessary to establish the need for higher initial dosing in pediatric patients.
Conflict of Interest
None
Funding Information
N/A
Ethical Statements
Current study was approved by REC-Riphah Institute of Pharmaceutical Sciences (RIPS) Approval Board for Human/Animal Studies with IRB reference number REC/RIPS-LHR/2023/721
Acknowledgement
N/A
Author Contributions
I. conception and design: All authors
II. data collection and assembly: All authors
III. data analysis, manuscript writing: All authors
All authors have approved this manuscript.