INTRODUCTION
Lung cancer accounts for around 150,000 deaths annually and is the leading cause of cancer-related mortality while being the second most common cause of cancer in the United States.1 Given its status as the leading cause of cancer death, there is an urgent need to identify new treatment options and improve our current therapies for this condition. The management of non-small cell lung cancer (NSCLC) has experienced a revolution thanks to the development of molecularly targeted therapies that have improved response rates and duration of response in many patients. It is estimated that approximately half of the patients with NSCLC harbor activating mutations, including alterations in EGFR in 15.6-22%, KRAS in 25%, ALK in 1.9-8.5%, ERBB2 in 2.4%, and more, depending on the population studied.2–4 These changes provide attractive targets for our growing armamentarium of oncogene targeted therapy. Recent and ongoing studies have shown an amazing ability to improve our outcomes for patients with newer TKIs targeting EGFR mutations and ALK rearrangements, as well as open new avenues of therapy for patients with other alterations, such as KRAS G12C mutations, MET exon 14 skipping, and RET rearrangements, and more. In this review, we outline the key clinical trials that guide our current molecularly targeted management of NSCLC.
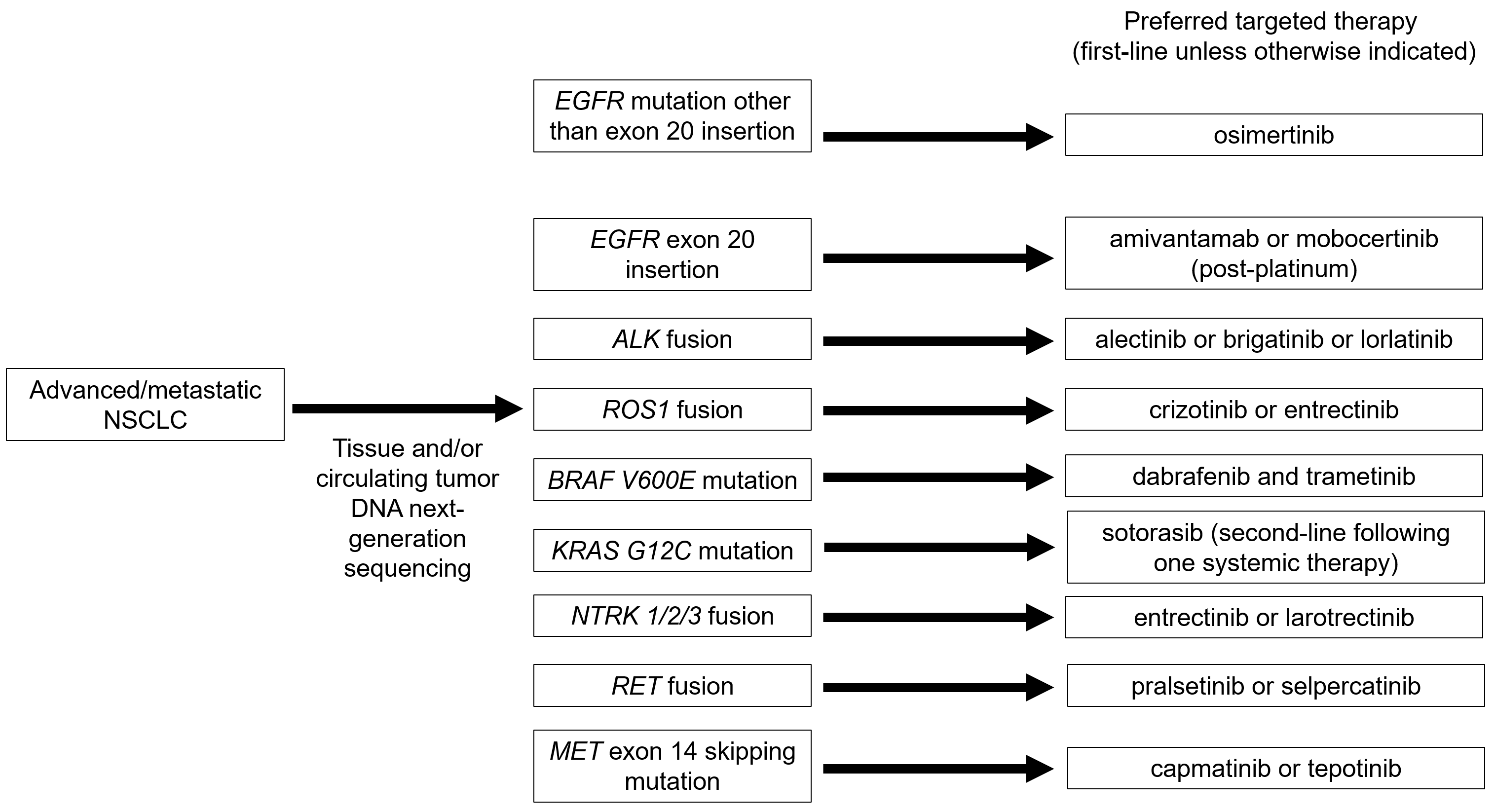
EGFR exon 19 deletions and L858R mutations
There are several options for the treatment of NSCLC with EGFR exon 19 deletions or L858R mutations. The preferred agent in this class is osimertinib, which received this status based on results from the FLAURA study.5,6 This trial compared osimertinib 80 mg daily with standard EGFR-tyrosine kinase inhibitor (TKI) therapy, involving gefitinib at 250 mg daily or erlotinib at 150 mg daily, in the first-line setting. With 556 patients, median overall survival (OS) with osimertinib was 38.6 months (95% Confidence interval (CI), 34.5-41.8) compared to 31.8 months (95% CI 26.6-36.0). This comparison was found to be statistically significant, with a hazard ratio (HR) of 0.046 (95% CI, 0.64-1.00). The rates of grade 3 or higher adverse events were 32% in the osimertinib group and 41% in the EGFR-TKI group, as reported by Soria et al. In an update in 2020, Ramalingam et al. reported 42% and 47%, respectively, for grade 3 or higher adverse events. Of note, patients receiving osimertinib had a longer duration of exposure, at 20.7 versus 11.5 months, respectively.
Other potential options for first-line therapy of patients with NSCLC with EGFR exon 19 deletions or L858R mutations include erlotinib,7–9 afatinib,10–14 gefitinib,15 dacomitinib,16,17 erlotinib plus ramicirumab,18 and erlotinib plus bevacizumab.19 Results from trials demonstrating the efficacy of these agents can be found in Table 1. Notably, combination therapy appears to have a median progression-free survival (PFS) more comparable to what is found in the FLAURA study, with erlotinib 150 mg daily plus ramucirumab showing a 19.4 month (95% CI, 15.4-21.6) median PFS compared to 12.4 months (95% CI, 0.46-0.76) for erlotinib.18 This was statistically significant, with a HR of 0.59 (95% CI, 0.46-0.76) and p<0.0001. Serious adverse effects were more likely in the combination group, with 29% versus 21% experiencing these, respectively. Median overall survival data for this study has not yet been reported.
EGFR exon 20 insertion
A couple recent studies have led to the accelerated approvals of amivantamab and mobocertinib for the treatment of NSCLC with EGFR exon 20 insertion. The phase I CHRYSALIS study treated patients who progressed following platinum chemotherapy with amivantamab 1400 mg weekly for the first four weeks, followed by the same dose every two weeks.20 This study showed an ORR of 40% (95% CI, 29-51) and a median PFS of 8.3 months (95% CI, 6.5-10.9). Median OS was 22.8 months (95% CI, 14.6-NR). Grade 3 or higher adverse events were experienced by 35% of the safety population and 39% of those treated with the recommended phase 2 dose. Infusion-related reactions were common but generally isolated to the first two doses of treatment and can be managed with premedication and lowering of infusion rate.
Zhou et al. recently reported the results of a pooled phase I/II study evaluating the efficacy of mobocertinib 160 mg daily in patients with platinum-pretreated NSCLC and EGFR exon 20 insertion.21 These patients showed an ORR of 28% (95% CI, 20-37), and a median PFS of 7.3 months (95% CI, 5.5-9.2). The median OS for this group was 24.0 months (95% CI, 14.6-28.8). Grade 3 or higher adverse events were experienced in 69% of patients.
ALK fusion
Several second- and further-generation TKIs have demonstrated efficacy in NSCLC with ALK fusions, leading to no defined preferred agent. The ALEX study evaluating alectinib 600 mg BID in the first-line setting in patients with ALK fusions has demonstrated an impressive overall survival on this therapy, with the median not reached, compared to 57.4 months (95% CI, 34.6-NR) with crizotinib 250 mg BID.22,23 The HR for this comparison was 0.67 (95% CI, 0.46-0.98). The ORR was 82.9% (95% CI, 76.0-88.5) in patients receiving alectinib compared to 75.5% (95% CI, 67.8-82.1), though this difference was not found to be statistically significant. The median PFS did show a statistically significantly improved median PFS at 34.8 months (95% CI, 17.7-NE) compared to 10.9 months (95% CI, 9.1-12.9). The HR for this comparison was 0.43 (95% CI, 0.32-0.58), with p<0.0001. The frequency of grade 3 or higher adverse events were reported by Peters et al. as 41% with alectinib and 50% with crizotinib in 2017. In a 2020 update, Mok et al. reported similar rates between the groups, at 52.0% for alectinib and 56.3% for crizotinib.
The ALTA-1L study compared brigatinib 180 mg daily to crizotinib 250 mg BID in first-line treatment with patients with ALK fusions.24,25 This study demonstrated an ORR of 74% (95% CI, 66-81) for brigatinib compared to 62% (95% CI, 53-70) for crizotinib. This was statistically significant, with a HR of 1.73 (95% CI, 1.04-2.88). Brigatinib had a median PFS of 24.0 months (95% CI, 18.5-NR) compared to 11 months (95% CI, 9.2-12.9) with crizotinib. Median OS has been reported as a HR of 0.92 (95% CI, 0.57-1.47), with a lack of statistical significance, given p=0.771. Patients experienced grade 3 or higher adverse events at a rate of 73% in the brigatinib group and 61% in the crizotinib group.
Provocative findings have been reported from the CROWN study, in particular for patients with CNS metastasis.26 Lorlatinib 100 mg daily was compared to crizotinib 250 mg BID. The ORR with lorlatinib was 76% (95% CI, 68-83) compared to 58% (95% CI, 49-66) for crizotinib. This comparison has an OR of 2.25 (95% CI, 1.35-3.89). The median PFS for lorlatinib was not reached and 9.3 months (95% CI, 7.6-11.1) for crizotinib. This difference was statistically significant, with a HR of 0.28 and p<0.001. Median OS has not yet been reported, but the investigators did report a HR of 0.72 (95% CI, 0.41-1.25) for this metric. Grade 3 or higher adverse effects occurred in 72% of lorlatinib patients and 56% of crizotinib patients. Table 2 serves to summarize these and subsequent studies discussed leading to the approval of targeted agents for molecularly altered NSCLC.
ROS1 fusion
Results from several phase I and II studies have guided the management of NSCLC with ROS1 fusion. Dziadziuszko et al. summarized three such studies which explored the response of patients who were ROS1-inhibitor naive to entrectinib ≥600 mg daily.27 Patients who received this treatment had an ORR of 67.1% (95% CI, 59.3-74.3). Median PFS was 15.7 months (95% CI, 11.0-21.1). median OS was immature at the time of publication.
The PROFILE 1001 study evaluated the use of crizotinib 250 mg BID in ROS1-inhibitor naive patients.28,29 The ORR in this population was 72% (95% CI, 58-83). The patients had a 19.3 month (95% CI, 15.2-39.1) median PFS and median OS of 51.4 months (29.3-NR). Grade 3 adverse effects were experienced by 36% of these patients.
Lim et al. evaluated ceritinib 750 mg daily in ROS1-inhibitor naive patients with ROS1-rearranged NSCLC.30 The ORR in this cohort was 62% (95% CI, 45-77). The median PFS in this group was 9.3 months (95% CI, 0-22). The median OS was 24 months (95% CI, 5-43). Grade 3 or higher adverse events affected 37% of patients in this study.
BRAF V600E mutation
A combination of dabrafenib and trametinib has been evaluated for NSCLC with BRAF V600E mutation in the first-line setting.31 In this phase II study, patients were treated with dabrafenib 150 mg BID and trametinib 2 mg daily. The ORR in this study was 64% (95% CI, 46-79). The patients receiving this combination had a median OS of 24.6 months (95% CI, 12.3-NE) and median PFS of 14.6 months (7.0-22.1). Grade 3 or higher adverse effects were experienced in 69% of patients.
KRAS G12C mutation
Sotorasib has recently gained accelerated approval for the treatment of KRAS G12C-mutated NSCLC in the post-chemotherapy, and optimally post chemoimmunotherapy, setting. The CodeBreaK100 study provided the data to support its use in this indication.32,33 In this study, patients received sotorasib 960 mg daily in patients who had progressed on immunotherapy and/or platinum-based chemotherapy. The ORR was 37.1% (95% CI, 28.6-46.2). Patients showed a median PFS of 6.8 months (95% CI, 5.1-8.2). The median OS was 12.5 months (95% CI, 10.0-NE). Grade 3 treatment-related adverse events affected 19.8% of patients, and one had a grade 4 adverse event. Of note, the use of proton pump inhibitors with sotorasib may substantially reduce drug levels and should be avoided.
NTRK 1/2/3 fusion
Larotrectinib and entrectinib are options for therapy in NSCLC patients with NTRK 1/2/3 fusions. Lin et al. pooled results from the NAVIGATE and NCT02122913 studies and showed that 20 patients with NSCLC and NTRK fusions treated with Larotrectinib 100 mg BID had an ORR of 73% (95% CI, 45-92).34,35 These patients had a median OS of 40.7 months (95% CI, 17.2-NE). Two patients (10%) experienced treatment-related grade 3 adverse events.
Doebele et al. evaluated the use of entrectinib in patients with advanced or metastatic NTRK fusions in a combination of phase I and II trials.36 Of the 54 patients, 10 had NTRK fusion NSCLC. These patients showed an ORR of 70% (95% CI, 35-93). Median OS for the entire cohort, not just the NSCLC patients, was 21 months (95% CI, 14.9-NE). Serious treatment-related adverse events affected 10% of the NTRK fusion-positive patients and 9% of the overall safety population.
RET fusion
Selpercatinib and pralsetinib have recently gained accelerated approval for the management of RET fusion NSCLC. Selpercatinib was evaluated in patients with prior platinum-based chemotherapy or without prior treatment in the LIBRETTO phase I/II study.37 The phase II dose was selpercatinib 160 mg BID. The patients with prior platinum-based chemotherapy had an ORR of 64% (95% CI, 54-73). This cohort had a median PFS of 16.5 months (95% CI, 13.7-NE). In the treatment naïve cohort, the ORR was 85% (95% CI, 70-94). Median OS was not reached in this group, and neither group reached median OS. Grade 3 or higher treatment-related adverse events were experienced by 28% of patients.
The use of pralsetinib in patients with RET rearrangements was tested in the ARROW study.38 Similar to LIBRETTO, this study was a phase I/II evaluation of patients treated with pralsetinib, with the phase II dose of 400 mg daily. Patients were separated into prior platinum-based chemotherapy and treatment naïve groups. The ORR for these groups were 61% (95% CI, 50-71) and 70% (50-86), respectively. Median PFS was 17.1 months (95% CI, 12.7-18.4) for the platinum-treated group and 9.1 months (95% CI, 6.1-13.0) in the treatment naïve group. Grade 3 or worse treatment-related adverse events affected 48% of patients in the NSCLC safety population.
MET exon 14 skipping mutation
Capmatinib and tepotinib have been approved by the FDA for the treatment of advanced NSCLC with MET exon 14 skipping mutations. The GEOMETRY trial provided support for capmatinib’s approval for this indication.39 In this phase II study, patients with this mutation were binned into cohorts based on prior treatment regimens and received capmatinib at a dose of 400 mg BID. The ORR for treatment naïve patients receiving this therapy was 68% (95% CI, 48-84). The ORR for patients with one or two prior lines of therapy was 41% (95% CI, 29-53). Median PFS for these groups were 12.4 months (95% CI, 8.2-NE) and 5.4 months (95% CI, 4.2-7.0), respectively. Grade 3 or higher adverse effects were experienced by 67% of patients.
Tepotinib was studied for NSCLC with MET exon 14 skipping mutations in the phase II VISION study.40 Enrolled patients were allowed to have up to two prior lines of therapy. The ORR for the treated population was 46% (95% CI, 36-57). The median PFS was 8.5 months (95% CI, 6.7-11.0). The median overall survival data was not mature, but it was reported as 17.1 months (95% CI, 12.0-26.8). Topotinib-related grade 3 or higher adverse events occurred at a frequency of 28%.

CONCLUSION
The impressive studies above have provided exciting improvements for the management of patients with molecularly-altered NSCLC. Importantly, they have provided hope for our patients with new and effective first- and subsequent-line options for their cancer. Notably, the pace of approvals of these agents seems to be quickening, with several gaining accelerated approval over the past couple of years. Future studies will attempt to refine and expand on these options to continue pushing to improve outcomes for patients with NSCLC.
FUTURE DIRECTIONS
The continued success and growth of molecularly directed therapy will rely on refining treatments for current targets, developing effective treatments for known targets without currently approved treatments, and identifying new molecular targets for patients with advanced or metastatic NSCLC.
Agents targeting HER2 are likely to be added as the next wave of targeted therapies available to clinicians to treat their advanced NSCLC patients. Trastuzumab Deruxtecan has been granted breakthrough FDA designation based on results from the currently active DESTINY-Lung01 trial.41 This trial showed a 55% ORR (95% CI, 44-65), median PFS of 8.2 months (95% CI, 6.0-11.9), and median OS of 17.8 months (95% CI, 13.8-22.1) in patients refractory to standard treatment. Similarly, poziotinib has been granted FDA fast track designation for patients harboring HER2 exon 20 mutations based on findings from a phase II trial demonstrating an ORR of 58% (95% CI, 40.9-73.0).42
The promising progress of recent years of molecularly targeted therapy in the NSCLC field will hopefully serve as a harbinger for continued discovery that will improve quality and duration of life for our patients.
Conflict of Interest
Dr. Schokrpur does not have any conflict of interest, including no relevant financial interests, activities, relationships, or affiliations.
Dr. Patel receives scientific advisory income from: Amgen, AstraZeneca, BeiGene, Bristol-Myers Squibb, Certis, Eli Lilly, Jazz, Genentech, Illumina , Merck, Pfizer, Rakuten, Signatera, Tempus
Dr. Patel’s university receives research funding from: Amgen, AstraZeneca/MedImmune, Bristol-Myers Squibb, Eli Lilly, Fate Therapeutics, Gilead, Iovance, Merck, Pfizer, Roche/Genentech, SQZ Biotechnologies
Funding information
Dr. Schokrpur received an honorarium in the amount of $2000 for this work.
Ethical statements
N/A
Acknowledgement
N/A
Author contributions
- SS and SP: conception and design,
- SS and SP: data collection and assembly
- SS and SP: data analysis, manuscript writing
All authors have approved the manuscript.