Background
Neuroendocrine tumors (NETs) arise from enterochromaffin or Kulchitsky cells which are widely dispersed throughout the body and thus, can form in different locations such as the gastrointestinal (GI) tract, pancreas, and lungs. The incidence of NETs has been on the rise with bronchopulmonary NETs (BPNETs) being the second most common, comprising 20-30% of all NETs.1,2 This trend is likely attributed to increased awareness of NETs, improved radiographic technology that is more widely available, and increased screening for cancers. Based on the World Health Organization (WHO) 2015 classification, the four histologic variants of lung NETs include small cell lung carcinoma (SCLC), large cell neuroendocrine carcinoma (LCNEC), and carcinoid tumors which are further divided into typical carcinoid (TC) and atypical carcinoid (AC) tumors.3,4 For this review, BPNETs will refer to TC and AC tumors.
While they fall under the umbrella of neuroendocrine neoplasms, SCLC and LCNEC are collectively called poorly differentiated high-grade neuroendocrine carcinomas, significantly different from well-differentiated low-grade TC and intermediate-grade AC tumors in terms of their clinical behavior and epidemiological, genetic, and molecular findings.5 BPNETs are often diagnosed in patients between 40-60 years of age and without a history of smoking, suggesting different underlying biology and etiological factors compared to other lung cancers.2 Besides various cytological and histologic characteristics including the extent of necrosis, Ki-67 nuclear expression is useful in separating high-grade SCLC and LCNEC from BPNETs.3 For further identification, the mitotic count is key in differentiating TC from AC tumors and should be performed per 2mm2 in the areas of highest activity.3,4 While TC tumors are characterized by less than 2 mitoses/2mm2 and absence of necrosis, AC tumors have 2-10 mitoses/2mm2 with presence/absence of necrosis. These findings are summarized in Table 1.
The WHO classification also recognizes diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH) as a preinvasive lesion. DIPNECH is rare, manifested as hyperplasia of neuroendocrine cells which may be diffuse, or in rows or clusters, and is usually confined to the bronchial or bronchiolar epithelium. When proliferation of neuroendocrine cells extends beyond the epithelium, crossing the basement membrane into the stroma, it forms tumorlets. These lesions are often discovered incidentally as peribronchiolar nodular aggregates and are morphologically identical to TC tumors but measure less than 5 mm in size.6 DIPNECH and tumorlets can co-concurrently be seen with BPNETs.
Up to 64% of BPNETs are located centrally with a higher rate noted in TC tumors in some studies, which makes patients more prone to obstructive respiratory symptoms compared to those with peripherally located BPNETs, which are often discovered incidentally.7–9 Patients can present with symptoms such as coughing, hemoptysis, wheezing, chest pain, and recurrent pneumonia, and they are sometimes repeatedly treated for common respiratory diseases such as chronic obstructive pulmonary disease and asthma until another pathological process is suspected, leading to a delay in diagnosis.
In about 90% of the cases, BPNETs are diagnosed as solitary lesions.7 Variable rates of lymph node involvement at the time of diagnosis have been reported. Overall, a higher rate is observed in AC tumors, with one study reporting lymph node involvement in 57% of patients with AC compared to 14% in patients with TC tumors.7,10–12 Besides intrathoracic spread, the most common sites of distant metastasis are bone and liver, noted in about 20% of patients with AC and 3% with TC tumors.2,11 Metastasis to the central nervous system has been reported as well and was seen in patients with AC tumors.13
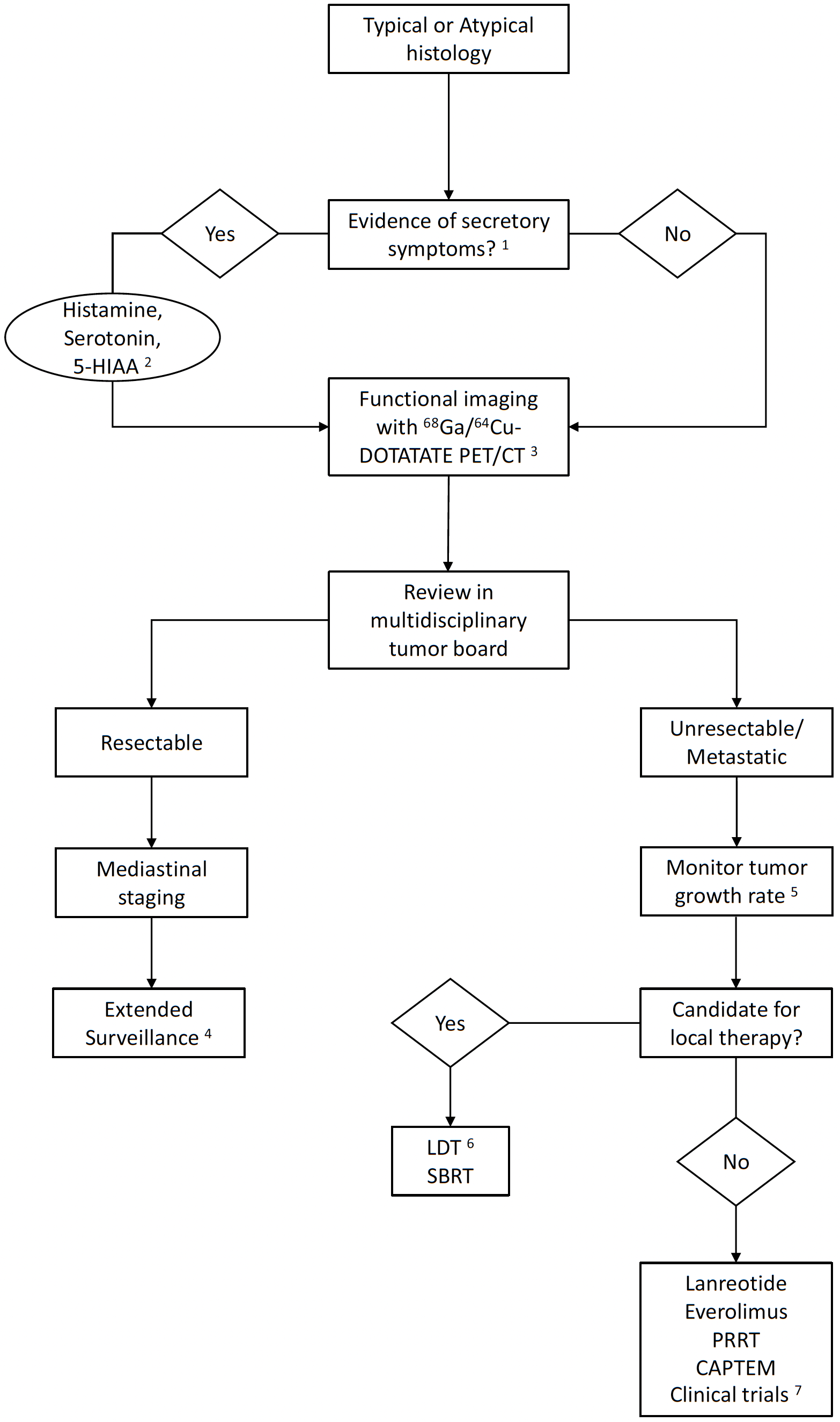
In 2-5% of cases, the tumor may be functional and present with carcinoid syndrome. This has been noted especially in the presence of liver metastases but is less common in BPNETs compared to patients with GI NETs.11,14,15 Cushing’s syndrome is also rarely found, however, up to 40% of patients with ectopic Cushing’s have been reported to have a BPNET.16 Other rare presentations that have been reported include acromegaly and hypoglycemia secondary to tumors secreting growth hormone-releasing hormone and insulin-growth factor 2.17,18 There is limited utility of routine baseline plasma chromogranin A (CgA) testing in patients with BPNETs and poor correlation with disease status.19 CgA can also be falsely elevated with renal impairment, atrophic gastritis, and the use of proton pump inhibitors.20 Other biochemical tests such as histamine, urine 5-hydroxyindoleacetic acid (HIAA), cortisol, and adrenocorticotropic hormone (ACTH) should be obtained as clinically indicated.
The initial gold standard radiological test is contrast-enhanced computed tomography (CT), which identifies both the primary lesion and intrathoracic lymphadenopathy. BPNETs usually range in size from 2-5 cm and may either be purely intraluminal appearing as a polypoid lesion or purely extraluminal. More frequently though, they are partially intraluminal with an extraluminal component, referred to as iceberg morphology.21,22 Since DIPNECH primarily affects the bronchial wall, it presents with CT changes characteristic of airway-related diseases. Bilateral mosaic attenuation, air trapping, and multifocal micronodules on expiratory CT have been reported.23 Multiphase CT or magnetic resonance imaging (MRI) of the abdomen should also be used to evaluate for metastasis to the liver and bone.
The role of positron emission tomography (PET)/CT in the diagnosis of NETs has evolved significantly over the years. NETs are known to overexpress somatostatin receptors (SSTRs), which provides a molecular basis for functional imaging and therapeutic application of somatostatin analogs (SSAs). In one study, investigators studied the expression of SSTR1 to SSTR5 in 178 BPNETs and found that 75% of tumors expressed SSTR2.24 Therefore, besides Fluorine 18-fluorodeoxyglucose (18F-FDG), SSAs such as DOTANOC, DOTATOC, DOTATATE labeled with 68Ga and 64Cu are now widely used as part of the standard diagnostic workup. 68Ga and 64Cu-DOTATATE are now both approved by the Food and Drug Administration (FDA) and available for diagnostic purposes in the US. When available, these are preferred over somatostatin receptor scintigraphy (SRS) due to higher sensitivity.25 Not surprisingly, PET/CT using 68Ga-DOTATOC has been reported to be superior to 18F-FDG in diagnoses of TC. The reverse has been observed in patients with AC.26,27 This is because AC tumors have a higher grade than TC tumors and are, therefore, hypermetabolic and more aggressive. The degree of uptake on 8F-FDG PET/CT can help provide prognostic information and uptake on PET/CT with somatostatin analogs is a prerequisite for peptide receptor radionuclide therapy (PRRT).28
To obtain a histologic diagnosis, bronchoscopy for central tumors and either an endoscopic transbronchial or CT-guided transthoracic biopsy for peripheral tumors is performed. When there is evidence of distant metastasis, a metastatic lesion easier to access may be biopsied instead of the primary lesion. Since there is not a staging system that has been designed specifically for BPNETs, the Tumor-Node-Metastasis (TNM) model for lung cancers in the 8th edition of the American Joint Committee on Cancer (AJCC) is used.29
The overall 5-year survival rate of patients with BPNETs has been reported to be 73.5% with rates as high as 92% reported in patients with TC tumors.2,9,11,12 Nodal involvement and presence of distant metastases are independently associated with a negative impact on survival.30,31 Absence of nodal involvement, referred to as N0 disease, confers excellent prognosis compared to patients with N1 or N2 disease with 5-year survival rates as high as 97%.9,10 While not validated by the WHO for BPNETs, Ki-67 was found to be an independent prognostic marker in one study.31
Treatment of BPNETs requires a multidisciplinary approach and given their rarity, referral to a tertiary academic NET center is preferred. There are several factors to be considered in optimal management of BPNETs such as tumor size, location, presence of nodal/distant metastasis, comorbidities, presence of hormonal symptoms, and previous lines of therapy. For patients with metastatic disease, an assessment of the tumor growth rate based on serial imaging is important. Systemic treatment is reserved for when there is clinical or radiographic progression, uncontrolled or worsening symptoms or if there is high disease burden, especially in the liver. In this review, we summarize current literature including guidelines from North American Neuroendocrine Tumor Society (NANETS), The European Neuroendocrine Tumor Society (ENETS), and National Comprehensive Cancer Network (NCCN), and provide updates on recent developments in the management of BPNETs.
Management
1. Surgery and adjuvant treatment
Surgical resection, when feasible, remains the initial treatment of choice for localized disease and provides a chance of cure. The choice of technique and extent of surgical resection depends on tumor location, size, pre-operative degree of suspicion for nodal involvement, and whether it is a TC or an AC tumor. Pre-operative histologic diagnosis is usually known, however, if only a small specimen was obtained during initial biopsy, it may become challenging to differentiate between TC and AC tumors.10,32 In some cases, patients are taken directly to surgery or rarely, these tumors may be incidentally discovered on surgical specimens post-operatively. Overall, the guiding principles for surgical resection of non-small cell lung cancer (NSCLC) are applied for BPNETs with lobectomy being the gold standard, however with special considerations due to their low grade and indolent clinical behavior. Minimally invasive and parenchymal sparing techniques have become increasingly preferable when possible. The choice of lung-sparing surgical technique is often dependent on the institution and surgeon’s training and experience.
For peripherally located TC tumors measuring less than 2 cm, lung-sparing surgery is an option if an R0 resection can be achieved.33 However, for larger peripheral tumors and when there is concern for AC, patients with adequate pulmonary reserve should be considered for a lobectomy.34 Similarly, for centrally located tumors, most of which are TC, parenchymal-sparing resections including bronchoplastic procedures, bronchial sleeve, or sleeve lobectomy are preferred over pneumonectomy or bilobectomy. In studies with patients with N0 TC tumors, lobectomy versus sublobar resection yielded similar 5-year overall survival (OS) rates.35,36 In the same population, a clear survival advantage was noted for patients who underwent surgery versus observation. However, the 5-year disease-specific survival was still high at 88% in patients who underwent observation-only, suggesting it may be reasonable to consider this approach in patients who are at high risk for surgery-related morbidity and mortality.36 In one study, due to a high rate of lymph node involvement and multicentric forms noted in their patients, authors recommended an aggressive approach with lobectomy and lymph node dissection for all patients.10 Typically, a 5 mm negative margin is considered appropriate.
Lymph node upstaging has been found to be a strong independent predictor of OS.35 Systemic hilar and mediastinal lymph node dissection is, therefore, highly advocated in patients due to this reason and high rates of nodal involvement, especially in patients with AC tumors. Pre-operative mediastinal staging should especially be considered in patients with clinical concern for N1 or N2 disease or peripherally located N0 tumors but with suspicion for AC.34
In cases of intraluminal BPNETs without an extraluminal component, endobronchial mechanical or laser-assisted resection can be considered.37,38 In one study, patients with purely intraluminal BPNETs measuring less than 20 mm in diameter on CT were noted to be good candidates despite histological grade with procedure-associated bleeding in 9% of patients. Interestingly, endobronchial treatment was also successfully performed in 28% of patients with possible extraluminal disease noted on CT.39 In a small study, cryotherapy was performed as adjunctive treatment to endobronchial resection and was noted to be safe and effective with only 1/18 patients noted to have recurrence after seven years. In another study, presurgical endoscopic resection of large tissues specimens performed in nine patients allowed for more accurate histological diagnosis and assessment of tumor base and improvement in respiratory status with potential impact on the ability to perform a lung-sparing surgery.40
There are no large prospective studies to evaluate the role of adjuvant therapy for BPNETs. The NCCN, NANETS, and European Society of Medical Oncology (ESMO) have varying recommendations for adjuvant chemotherapy of BPNETs. NCCN recommends against adjuvant treatment for stage I and II BPNETs but recommends considering it for stage IIIA patients based on expert opinion. Specifically, they recommend considering either a platinum doublet (cisplatin/carboplatin + etoposide) or temozolomide for patients with stage IIIA disease with either intermediate grade and negative margins or positive margins irrespective of histology. However, they also state the lack of data to support this recommendation.41 Chemotherapy may also be combined with radiation if considered appropriate. ESMO recommends the consideration of adjuvant treatment for patients with AC and nodal disease. NANETS recommends against adjuvant treatment.33,42 Current literature does not suggest a consistent benefit in OS with adjuvant chemotherapy.43 Some authors have recommended its use in a subset of patients with adverse pathologic features and lymph node involvement based on a trend towards improved OS compared to published literature, however, this evidence is limited.44,45 In fact, in one study, in patients with TC tumors, adjuvant treatment was associated with significantly worse outcomes46 and should, therefore, not be used outside of a clinical trial.
For patients who are not surgical candidates or have unresectable locally advanced BPNET, NCCN recommendations are based on tumor grade.41 For intermediate grade stage III A/B/C BPNETs, platinum-doublet chemotherapy with or without radiation may be considered. For low-grade stage III A/B/C BPNETs, observation versus other systemic therapy options discussed under medical management below may be considered. If patients with intermediate-grade stage III A/B/C BPNETs are poor candidates for aggressive treatment with chemotherapy, other systemic therapies may be used with or without radiation. SSA are overall well-tolerated and can manage symptoms and also provide an anti-proliferative effect. Radiation alone may be used for palliation if systemic therapy is contraindicated.
2. Medical management
The goal of systemic therapy in the treatment of NETs includes control of both symptoms and tumor growth. Systemic treatment options for BPNETs include SSAs, targeted therapies, chemotherapies, PRRT, and clinical trials. These treatment options are used for patients with unresectable or metastatic disease. The sequencing of these treatment options is not well defined. An individualized patient-centered approach based on clinical status and radiological findings is essential in formulating an optimal treatment plan.
a) Somatostatin analog therapy
Treatment with SSAs including lanreotide autogel (LAN) and octreotide long-acting release (LAR) is well tolerated and effectively manages symptoms as well as provides antiproliferative effect in patients with NETs. SSAs are recommended by NANETS, ENETS, and NCCN in the management of BPNETs. The PROMID and CLARINET study established SSAs as first-line monotherapy in patients with NETs of the GI tract and pancreas.47,48 In the PROMID study, 85 patients with well-differentiated metastatic midgut NETs received either placebo or octreotide LAR 30 mg every month. There was a statistically significant improvement in median time to tumor progression (TTP) of 6 months in placebo versus 14.3 months in the treatment arm.48 In the CLARINET study, 204 patients with advanced gastroenteropancreatic (GEP) NETs received either placebo or LAN 120 mg every 28 days. There was a statistically significant improvement in progression-free survival (PFS) with median PFS not yet reached at the time of publication in the treatment arm compared to 18 months in the placebo arm.47 Results of the open-label extension of the CLARINET study revealed a median PFS of 38.5 months.49 None of these studies, however, included patients with BPNETs.
Three retrospective studies including patients with BPNETs who received SSAs either as first50,51 or first/subsequent52 line therapy have been published. The initial study that described the use of SSAs in first-line setting in BPNETs only was published in 2017, included 20 patients treated with octreotide LAR and 10 patients with lanreotide. Twenty-three out of 30 patients had AC tumors. Stable disease (SD) was observed in 87% of patients and partial response (PR) in one patient. The 5-year survival rate was 53% and the median PFS was 11.1 months.50 Another recent study published in 2021 included 31 patients with a fairly equal number of AC (17) and TC (14) tumors. This study demonstrated SD in 77.4% of patients with a median PFS of 28.6 months.51 The largest of these studies included 61 patients, 76% of whom received SSAs as first-line therapy. In this study, the median PFS was 17.4 months and the median OS was 58.4 months.52
Most recently, the findings from the phase III SPINET trial were presented at the 2021 NANETS symposium. This trial randomized patients with BPNETs to either LAN plus best supportive care versus placebo. Enrollment to the trial was stopped early due to slow accrual. A total of 77 patients were randomized and treated. In this trial, the median PFS was 16.6 months (95% CI, 11.3 to 21.9) in the treatment arm versus 13.6 months (95% CI, 8.3 to not calculable) in the placebo arm with a hazard ratio (HR) of 0.90 (95% CI, 0.46–1.88). Specifically, the median PFS was 21.9 months with treatment versus 13.9 months with placebo in patients with TC tumors and 13.8 months with treatment versus 11 months with placebo in patients with AC tumors.53
b) Targeted therapies
Targeted agents that have been studied in the treatment of BPNETs include everolimus, an oral inhibitor of the mammalian target of rapamycin (mTOR) pathway, and antiangiogenics such as sunitinib and pazopanib. Out of these, everolimus has the highest quality evidence to support its use in the treatment of BPNETs and was approved by the FDA in 2016 in this setting.
1) Everolimus
mTOR is a serine/threonine kinase, downstream of the phosphatidylinositol-3-kinase (PI3K)/Akt pathway, activation of which results in significant disturbance in controlling cell growth and survival. The role of this pathway in tumorigenesis, specific to NETs, has been demonstrated.54,55 Everolimus is a derivative of rapamycin and an inhibitor of this pathway. The pre-clinical data with human BPNETs in primary cultures treated with everolimus showed inhibition of mTOR complex 1 (mTORC1) and thus, was a promising therapeutic target.56 Everolimus was first approved in the treatment of advanced, progressive pancreatic NETs based on phase III data from the RADIANT-3 trial, published in 2011, which showed a median PFS of 11 months in patients who received everolimus at 10 mg daily versus 4.6 months with placebo.57 Matured data showed a non-statistically significant survival benefit of 6.3 months, which was attributed to a large crossover from the placebo arm.58
Shortly thereafter, the RADIANT-2 trial was published, which included patients with advanced NETs from any primary site, associated with carcinoid syndrome. Patients received either everolimus or placebo, both in conjunction with octreotide LAR monthly. The median PFS in the treatment arm was 16.4 months (95% CI, 13.7 to 21.2) compared to 11.3 months (95% CI, 8.4 to 14.6) in patients who received placebo and SSA with an HR of 0.77 (95% CI 0.59 to 1.00; p = 0.026).59 However, the final OS analysis was not consistent with these initial findings. The median OS was 29.2 months in the treatment arm versus 35.2 months in the placebo arm with an HR of 1.17.60 Several factors were speculated to influence these results including heterogeneous study population, crossover from the placebo group, unequal SSA use, and some patients who may not have needed to start aggressive therapy, which in turn may have led to more frequent adverse events. This study emphasized the importance of the “wait and watch” strategy as some patients may have indolent disease for years and could be monitored closely, reserving treatment options for time of progression. A sub-group analysis of the RADIANT-2 trial including 44 patients with BPNETs only was later published. Thirty-three of these patients had received everolimus and the median PFS was 13.63 months (95% CI, 5.55 to 14.29) in patients who received everolimus plus SSA versus 5.59 months (95% CI, 2.79 to 27.76) in placebo plus SSA, a 2.4 fold improvement, with an HR of 0.72 (95% CI, 0.31–1.68; p = 0.228). The authors also noted that 67% of the patients who received everolimus had minor tumor shrinkage compared to 27% in the placebo arm.61
Following this, results of the RADIANT-4 trial were published. This international trial enrolled 302 patients with advanced, progressive, well-differentiated, and non-functional (unlike RADIANT-2) NETs originating in the GI tract or lungs to receive either everolimus or placebo. The median PFS in the treatment arm was 11 months compared to 3.9 months in the placebo group with an HR of 0.48. Treatment was well-tolerated with infrequent grade 3 or 4 drug-related events, which included stomatitis, diarrhea, anemia, fatigue, and hyperglycemia.62 A post hoc analysis of the lung subgroup with 90 patients showed a median PFS of 9.2 months in the everolimus arm versus 3.6 months in the placebo arm with an HR of 0.5.63
To further study the role of the everolimus in treatment-naïve patients and its combination with SSA due to possible synergy secondary to their effects on the mTOR pathway, the ITMO trial was designed. This was a phase II study that enrolled 50 patients with NETs of multiple origins including 11 patients with BPNETs and received everolimus in combination with octreotide LAR. The overall response rate (ORR) was 18% with SD noted in 74% of patients.64 A 5-year update showed promising results with a median TTP of 33.6 months and the median OS of 61 months.65 The phase II LUNA trial was the only study to enroll patients with advanced, well-differentiated thymic and BPNETs only and had three separate arms, pasireotide alone, everolimus alone, or a combination of both. The median PFS was 8.5, 12.5, and 11.8 months in the pasireotide, everolimus, and combination group, respectively.66
The NCCN and ENETS guidelines recommend using everolimus in the first-line setting in patients with BPNETs who have progressive disease or high-tumor burden. Everolimus may be combined with SSAs, especially in patients with functional BPNETs. The initial dose is 10 mg and is typically reduced in increments of 5 mg or less depending on tolerability. Patients may develop resistance and while previous studies have identified resistance mechanisms, no agents with promising safety profiles have been developed to overcome these resistance pathways so far.54
2) Antiangiogenics
The data for the use of antiangiogenics in the treatments of BPNETs is not as robust. Sunitinib is used in the treatment of pancreatic NETs based on prospective trials67 but the results for BPNETs have not been impressive. In a phase II trial, sunitinib was prescribed at a dose of 50 mg/day for 4 weeks on followed by 2 weeks off. The trial enrolled 109 patients, including 14 patients with gastric and BPNETs. Among these patients, while the ORR was only 2.4%, 83% of patients had SD with 10.2 months of median TTP.68 In the phase II PAZONET study, a total of 44 patients with advanced NETs who had failed on other systemic therapies were enrolled, 5 of whom had BPNETs. The shorter median PFS of 3.4 months was noted in patients with lung and thymic NETs compared to 12.8 months in pancreatic NETs and 10 months in GI NETs.69 A combination of sorafenib and bevacizumab has been used but yielded unfavorable safety results.70 Bevacizumab has also been compared to pegylated (PEG) interferon alpha-2b, both used in combination with SSA in a phase II study. A total of 44 patients were enrolled including four with BPNETs. A higher PFS rate of 85% after 18 weeks of treatment was observed in the bevacizumab arm compared to 68% in the PEG interferon alpha-2b arm.71 Recently, in a phase III study, 198 patients with advanced extrapancreatic NETs, including 23 patients with BPNETs, were treated with either surufatinib or placebo. The median PFS in the treatment arm was 9.2 months versus 3.8 months in the placebo arm.72
c) Chemotherapy
Systemic chemotherapy is typically reserved for patients with metastatic and progressive BPNETs. Data for several different regimens has evolved over the years but needs to be interpreted with caution due to the often mixed population of primary tumors and the small number of patients with BPNETs in studies.
Initial studies dating back to 2001 demonstrated discouraging results. In a study with 31 patients with metastatic BPNETs, 7 of 7 patients progressed on streptozotocin and 5-fluorouracil (5-FU), while SD for up to 10 months was achieved in 2 of 2 patients treated with streptozotocin and doxorubicin.73 Subsequently, a phase II/III trial with 249 patients with advanced NETs including 22 patients with BPNETs compared 5-FU/doxorubicin with 5-FU/streptozotocin. There were no differences between 5-FU/doxorubicin and 5-FU/streptozotocin in terms of response rates and median PFS, however, 5-FU/streptozotocin was noted to be superior in median survival. Patients who progressed on either regimen crossed over to dacarbazine and a response rate of 8.2% was noted.74 Following this, 5-FU/streptozotocin was also combined with cisplatin and this combination resulted in a 25% response rate for non-pancreatic primary sites.75 In a subsequent trial, however, no added benefit of cisplatin to capecitabine/streptozotocin was noted.76 A patient with metastatic BPNET was also successfully treated with a combination of liposomal doxorubicin and capecitabine after progressing on cisplatin and etoposide. These combinations are not routinely used in practice for BPNETs.77
The platinum doublet combination used in the first-line setting for LCNEC and SCLC has shown to be beneficial only in a subset of patients with BPNETs, most likely secondary to their less aggressive biology and lower grade.78 In a retrospective analysis, 13 patients with metastatic BPNETs treated with etoposide and platinum combination showed a response rate of 23%, a disease control rate (DCR) of 57%, and a median PFS of 7 months.44 Similar responses were noted in another retrospective study where 23.5% of patients with metastatic BPNETs treated with etoposide and platinum combination were noted to have responses and had a median PFS of 7 months.13
Other platinum-based regimens such as 5-FU, leucovorin and oxaliplatin (FOLFOX), capecitabine and oxaliplatin (CAPOX), and gemcitabine and oxaliplatin (GEMOX) have also shown efficacy. In one retrospective analysis, 31 patients with grade 1/2 NETs, including 8 patients with BPNETs treated with one of these oxaliplatin-based regimens, were studied. The overall DCR was 70% and the median PFS was 14.1 months with no significant differences between Ki-67 subgroups of <5% and 5-20%.79,80 CAPOX was studied in 24 patients with metastatic NETs, 63% of whom were classified as grade 1/2 and 17% originated in the lungs. Out of these, 29% of patients achieved a PR and the median TTP was 9.8 months.81 In a phase II trial, 40 patients with advanced NETs were enrolled and treated with CAPOX, 27 of whom had well-differentiated tumors and 10 patients had NETs originating in the lungs. This regimen was found to be effective and was well tolerated.82 Among these, for patients with well-differentiated NETs, 30% had a PR and 38% had SD. In one study with BPNETs only, either GEMOX or FOLFOX was used in 45 patients including both treatment naïve and pre-treated patients, and showed similar outcomes with either regimen. The median PFS was 15 months and the median OS was 34 months.83 In a larger study with 78 patients with mainly grade 2 NETs, 19 of whom had BPNETs, patients received either CAPOX, GEMOX, or FOLFOX. The median PFS was 8 months and the median OS was 32 months.80 Single-agent metronomic 5-FU with octreotide LAR has also shown efficacy in a phase II trial, however, no patients with BPNETs were included in this study.84
Multiple studies with temozolomide both as monotherapy and in combination with other agents such as SSAs, bevacizumab, and capecitabine have been published. In a retrospective analysis of 31 patients treated with temozolomide, PR was noted in 14% and SD in 52% of patients. The median PFS was 5.3 months and the median OS was 23.3 months.85 Recently, results of ATLANT phase II trial were published, where 40 patients with progressive BPNETs and thymic NETs were enrolled and treated with LAN and temozolomide for 12 months. At 9 months, the DCR was 35% and the median PFS was 5.3 months.86 In a phase II study, temozolomide was combined with bevacizumab in patients with pancreatic and extra-pancreatic NETs, including 4 patients with BPNETs. Response rates were higher in pancreatic NETs with no PRs noted in extra-pancreatic NETs. However, SD was achieved in 74% of the patients and the median PFS was 7 months.87 Multiple studies with combination of capecitabine and temozolomide (CAPTEM) have shown promising results. Several retrospective analyses have reported a DCR of over 70%.88–91 In one study, the median PFS and OS were 13 and 68 months, respectively.91 A trend of better outcomes in patients with lower Ki-67 values was noted.88,90 MGMT methylation was associated with higher disease control and prolonged TTP.89 Interim analysis of a phase II study of patients with well-differentiated NETs treated with CAPTEM showed a median PFS > 22 months.92
d) Peptide Receptor Radionuclide Therapy (PRRT)
PRRT may be used in patients with metastatic BPNETs who have positive uptake on SSTR imaging, either PET/CT or SRS. High energy beta-emitting radionuclides, Ytrrium-90 (Y-90) or Lutetium-177 (Lu-177) are bound to SSAs such as DOTATOC and DOTATATE to reach and penetrate SSTR positive cells. The goal of treatment is disease control and palliation of symptoms. In a phase II study with 41 patients including 7 with BPNETs, 100% of patients with BPNETs achieved disease control with no progressive disease within the follow-up period.93 Subsequently, in a large phase II study with 1109 mixed population of NET patients, disease control was achieved in 39% of patients with a median survival of 94.6 months. In 84 patients with BPNETs, a morphologic response was noted in 28.6% of patients and clinical response in 38%. Tumoral uptake in the initial imaging study was an independent predictor of OS.94
In a retrospective study with 135 patients, 13% of whom had BPNETs revealed a median OS of 40 months from the date of first PRRT. Specifically, in patients with BPNETs, the median OS from first PRRT was 32.4 months and TTP was 18.6 months.95 In another retrospective study compromising of 114 patients with BPNETs treated with PRRT, the median PFS was 28 months and the median OS 58.8 months.96 Other retrospective analyses of patients with BPNETs have also revealed a median OS ranging between 40-42 months. Intense uptake (SUVmax > 5) on 18F-FDG PET/CT was associated with a poor response97 and high hepatic tumor burden and high CgA levels were noted to be negative predictors of survival.98
While it didn’t include patients with BPNETs, the results of the NETTER-1 trial are worth noting as they could potentially be extrapolated to other NETs. This trial enrolled patients with inoperable well-differentiated midgut NETs to receive either PRRT or octreotide LAR and showed a substantial prolongation of PFS in the PRRT arm.99 Matured data was recently published and showed a non-significant improvement in median OS to 48 months in the PRRT arm versus 36.3 months in the control arm, potentially due to large cross-over.100 A phase II trial that aims to assess PFS in patients with advanced or metastatic BPNETs treated with either PRRT or everolimus is currently underway [NCT04665739].
Patients need to be monitored for hematological and renal toxicities that are usually mild and transient but may sometimes result in permanent damage. In one study, 9.2% of patients experienced grade 4 to grade 5 permanent renal toxicity, 12.8% of patients developed transient grade 3 to 4 hematological toxicity, and 2 patients developed myelodysplastic syndrome and acute myeloid leukemia.94 Other studies including the NETTER-1 trial have reported lower rates of toxicities.96–99
Conclusions
While the mainstay for operable BPNETs is surgical resection, the role of different systemic therapies in the treatment of advanced/metastatic disease has evolved significantly over the years. We have summarized recommendations in a treatment algorithm (Figure 1). The timing of initiating treatment and choice and sequence of therapies is crucial. A multidisciplinary and patient-centered approach is necessary for optimizing a treatment plan.

Future directions
Management of BPNETs has come a long way and has seen rapid advancements in our understanding of its molecular biology, histopathological classification, diagnostic modalities, and treatment options. The next big challenge for us is to define the efficacy of these novel agents in BPNET specific clinical trials and define treatment sequencing based on prospectively conducted studies with meaningful clinical endpoints. The rarity of BPNETs often poses enrollment challenges but a concerted effort between industry and oncology cooperative groups is the only way forward in pursuing meaningful and much needed clinical studies.
Conflict of Interest
RAR: Consulting for Amgen, Ipsen, Novartis, Advanced Accelerator Applications, Curium, EMD Serono; Speaking Fees from Ipsen, Astra-Zeneca, Merck; Research Funding (to institution) from Merck, AADI Bioscience
AC: Consulting for Novartis, Ipsen, Lexicon, TerSera; Research Funding from NCI CTEP, BMS, Clovis Oncology, TerSera, EMD Serono, Nanopharmaceuticals, ECS Progastrin
Funding information
N/A
Ethical statements
N/A
Acknowledgement
N/A
Author contributions
Garima Gupta: conception and design, manuscript writing and proofreading
Robert A Ramirez: support to Garima Gupta
Aman Chauhan: support to Garima Gupta
All authors have approved the manuscript