



Introduction
Phalangeal foot fractures are a common lower extremity issue mainly associated with either an axial force (e.g., stubbing a toe) or crush-type injury (e.g., dropping a heavy object on it).1 Many factors can interrupt the five stages of bone healing resulting in non-healing fractures.1 Potential occult causes must also be ruled out if there is a protracted- time between a fracture and healing. Although rare, malignancy as a cause for non-healing fractures should be part of the differential diagnostic process.2 There is currently limited literature on adult non-healing phalangeal foot fractures, with none outside of pathologic metastatic fractures that were missed3 or fractures present in undiagnosed cancers, to guide health care practitioners practice in this area.4
A cancer diagnosis at times can be elusive especially breast cancer (BC) in younger women. BC in premenopausal women is rare with less than 5 % of breast cancer patients falling below the age of 35.5 BC in younger women (<35 y/o) is aggressive and also challenging to diagnose due to the density of breast tissue, the limited nature of diagnostic tests available, and the rarity of a BC in this age group.5 Formulating a distinction between healthy fibroglandular tissue and an early malignancy is perplexing, requiring close follow up of younger women reporting changes in breast tissue.5–7
BC at any age is known to readily metastasize to the bone with bone health being a primary concern during and after treatment.8 Theories have emerged suggesting that breast cancer cells affect both bone osteoblastogenesis and osteoclastogenesis before, during, and after treatment.9–12 Bone biomarkers have recently become a focus suggesting that invasive and metastatic breast cancer cells release and activate matrix metalloproteinase (MMP), a large class of proteinases that restrict bone remodeling.9–12 Handforth et al. (2018) describe how breast cancer cells produce Activin a known up-regulator of receptor activator of nuclear factor kappa (RANK) which promotes osteoclastogenesis and similarly Inhibin A & B, heterodimeric proteins, which regulate both osteoblastogenesis and osteoclastogenesis affecting bone turnover and healing. These theories firmly link breast cancer to bone issues and may assist us in understanding how untreated BC affects non-metastatic fracture healing. The aforementioned factors may contribute to a lack of bone remodeling, a known requirement for healing2 when BC is undiagnosed and untreated in women with a non-healing fracture. An extensive review of current published literature was unable to locate any research on the effects of bone healing, outside of pathological bone fractures, during or before initiation of chemotherapy for breast or other types of cancer.
Cancer treatment has evolved into a complex multimodal approach with chemotherapy before surgery (neoadjuvant chemotherapy) for large breast cancer becoming a standard therapeutic regime.7 The goal of therapy is twofold; one to shrink the cancer tumor to allow for less invasive surgery and two to eradicate any cancer cells that may have migrated to other areas in the body.7,8 Chemotherapy-induced bone loss is a concern though research into long-term effects is inconclusive.9 Theoretically, as the cancer tumor shrinks and dies with treatment, it will cease to release any substances, known and unknown, that regulate other body systems and functions like bone healing.
In this case, we describe how a non-metastatic, non-healing pharyngeal fracture in a young woman led to the diagnosis of a later-stage BC and that once chemotherapy was initiated, bone remodeling took place and the fracture healed. A continued protracted period to BC diagnosis may have resulted in an ongoing issue with non-healing in this case. Practitioners’ awareness of undiagnosed and untreated cancer as a potential issue in nonhealing fractures is explored through this case study.
Case Presentation
History
A 30-year-old Caucasian female presented to a foot clinic with a right foot phalangeal fracture. Seven weeks prior she reported trauma from dropping furniture on her big toe, resulting in swelling, tremendous pain, and difficulty with ambulation. Her primary care provider (PCP) prescribed the use of a walking boot. She came to the clinic because her toe “Did not seem to be getting any better.” She stated that none of her symptoms had subsided even though she remained in the walking boot, was resting, and following all of the other recommendations from her PCP.
Clinical Findings
A focused history and physical exam revealed no history of medications or other health issues except for the toe pain. She reported living an active lifestyle, including gym-based exercise, yoga, following a vegetarian diet, smoking abstinence, and social alcohol use. She stated that she was employed full-time as a social worker in a long-term care facility and had no known significant family history of any significant genetic health issues.
Upon observation, her right great toe had ongoing soft tissue swelling, nail and skin were intact. It was tender to the touch and guarding was noted upon examination. Pedal pulses were intact and equal bilaterally, with no neurological deficits noted. She had apparent discomfort when observed ambulating with and without the walking boot. Additional physical exam findings, of her lower extremities, were unremarkable.
Clinical Management
Initial radiography from January was reviewed and indicated a comminuted non-displaced fracture of the right distal phalanx with intra-articular extension. She was placed in an air-cast walking boot and was instructed to continue to modify her activities to allow for healing. A follow-up appointment was requested in 6 weeks. Upon follow up she remained in severe pain suggesting problems with bone healing. The reported ongoing pain was concerning, and follow-up films ordered in February (See X-rays #1 & #2) and again in March indicated a non-healing fracture.


On recall to the clinic, further history was assessed to rule out known causes associated with non-healing fractures. The patient reported no strict diet, medications, herbal supplements, or other health issues. However, during this visit, she stated that approximately ten months ago she noticed a change in her right breast. Her PCP examined her and sent her for a breast ultrasound (US). Upon follow up she was told not to worry about the breast; her US was negative revealing only normal fibroglandular tissue and no further follow-up was required. Since that time, she felt the breast lump had enlarged, and she noticed skin changes. The practitioner immediately referred her back to her PCP for follow-up; as it was suspected that there might be an occult systemic disease process interfering with her bone healing.
Differential diagnosis to guide practice
When evaluating pain and a non-healing fracture in younger patients’ questions must span the range of potential differential diagnoses. Could this be potentially related to malnutrition, diabetes mellitus, osteoporosis, Paget’s disease of the bone, peripheral vascular disease, thyroid/parathyroid dysfunction, or some other type of metabolic disease process such as malignancy?1,2,4–6
Follow up on reported breast issue
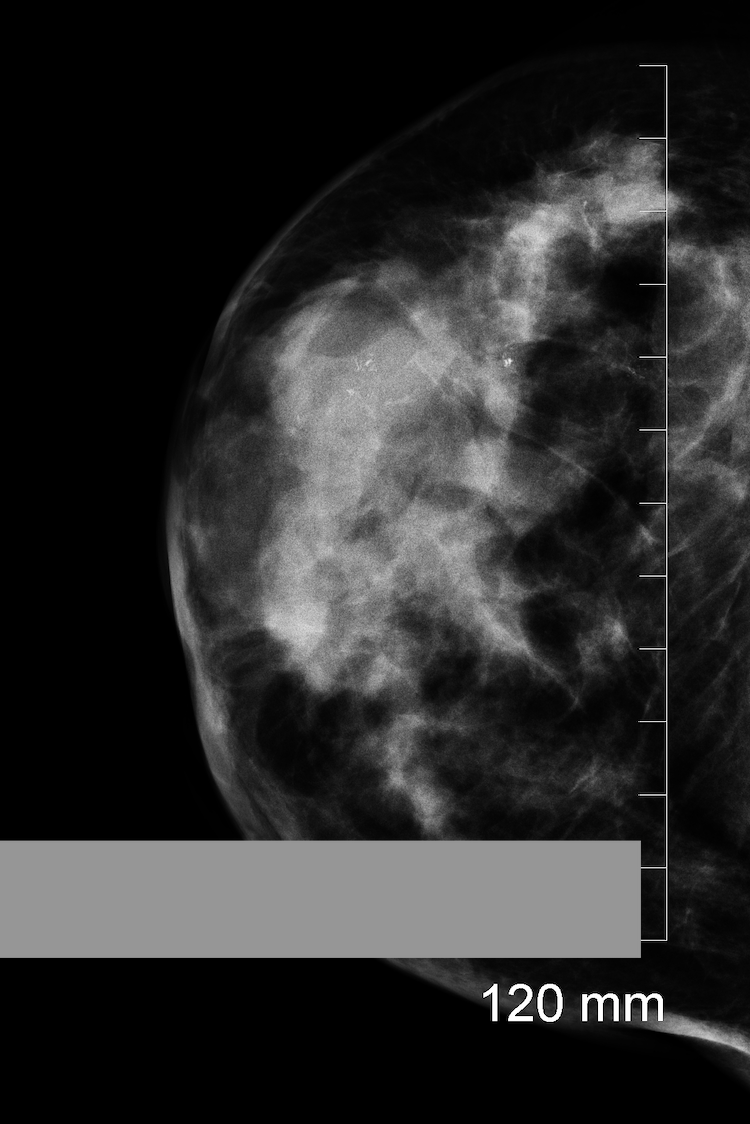
On physical re-examination by her PCP, she was found to have a significant mass in the upper outer quadrant of the right breast measuring approximately 11 cm in size. She also now had peau de orange changes and slight nipple retraction. The right breast also appeared to be decreased in size compared with the contralateral breast. As a result, an emergent mammogram was ordered (See mammogram) The mammogram was read as BI-RADS 4, highly suspicious for breast cancer, with a 7x11 cm mass with calcifications in the upper right quadrant increasing suspicion of malignancy. A follow-up US and a needle core biopsy were done. The result from the biopsy confirmed breast cancer.

She was immediately referred to medical oncology. A bone scan and bloodwork found no bone metastatic disease or indication of pathologic fractures. The only disease outside of the breast was suspicion of involved axillary lymph nodes. She began neoadjuvant chemotherapy staged as 3C (ycT4, N3, M0, ER+/PR-, HER2-) infiltrating lobular carcinoma. After two rounds of doxorubicin and cyclophosphamide, she returned to the foot clinic stating that her toe pain had resolved. The subsequent follow-up foot x-ray indicated a completely healed fracture (See X-rays #4 & #5). She was instructed to return to activity as tolerated while continuing her breast cancer protocol.


Discussion
This case highlights how a serendipitous great toe fracture with ongoing pain and lack of healing suggested a metabolic issue necessitating follow-up.4 It showcased the rare, but required, alternative differential diagnosis of cancer contributing to a non-healing fracture in a healthy young woman. A BC diagnosed because of a non-healing, non-metastatic fracture is undocumented in the current literature making this case unique.
Bone healing is a complicated process that varies from person to person. Cancer cells and their link to bone biomarkers, although in their infancy, are beginning to show promise in predicting which patients are at risk for metastatic bone disease and fracture.10 Although it cannot explicitly be stated that the initiation of chemotherapy directly resulted in her fracture healing, it is a plausible explanation. Once chemotherapy was initiated the potential cascade of excess MMP,12 Activin,10 and Inhibins10 would have been halted allowing bone remodeling to take place and her non-healing foot phalangeal fracture to heal.
Non-healing foot phalangeal fractures require close follow-up and investigation to ensure healing so that long-term consequences can be avoided, and mobility restored.1 The lack of proper follow-up screening tests for breast cancer in this young woman resulted in a later stage of breast cancer at diagnosis requiring more extensive interventions than if it was diagnosed earlier.8,13 Therefore, vigilant investigations of non-healing fractures in young women must include the differential diagnosis of undiagnosed breast cancer along with other systemic disease processes.
Ongoing Follow-up
Our patient completed neoadjuvant chemotherapy, with little change in her 3C staging, she underwent bilateral mastectomies with implant reconstruction, followed by radiation therapy. The extensive therapy noted was required due to the delay in her BC diagnosis. She is currently on leuprolide® and tamoxifen® in close follow-up. We remain cautiously optimistic about her future prognosis. She consistently had no indication of bone metastatic disease nor further issues with her healed great toe fracture.
Conclusion
In summary, a 30-year old female sustained an injury to her right great toe resulting in a phalangeal fracture. She presented within seven weeks of the injury with symptoms suggestive of a non-healing fracture. However, a red flag was raised after an additional six-weeks of symptoms and x-ray confirmation of an ongoing non-healing fracture. The resultant in-depth follow-up evaluation led to a late, lost-to-follow-up, breast cancer diagnosis. This case illustrated the importance of continued follow-up and assessment of nonhealing fractures with breast cancer or other malignancies considered as a differential diagnosis. As noted, initiation of chemotherapy coincided with this non-metastatic fracture healing, although it may be unrelated, it requires further investigation. Ongoing research into the effects of breast cancer and treatment, the ability of fractures to heal before treatment, and upon initiation of chemotherapy, along with the relationship to various cancer-affected bone biomarkers may shed light on the usefulness of these biomarkers in fracture healing in the future.
Conflict of Interest
None
Funding information
None
Ethical statements
Permission to use the clinical information, mammograms, and X-rays in the case study was given in writing by the patient to LF on which it is based. No ethical review is required for a case study.
Acknowledgement
N/A
Author contributions
i. LF and JF: conception and design,
ii. LF and JF: data collection and assembly
iii. LF and JF: data analysis, manuscript writing
All authors have approved the manuscript