
Introduction
Lung cancer remains the most common cause of cancer-related deaths worldwide with an estimated 2.2 million new cases each year.1 The predominant histological type, which accounts for approximately 85% of all cases, is Non-Small Cell Lung Cancer (NSCLC).2 Within this population, 40-55% have somatic mutations in the tyrosine kinase (TK) domain of EGFR.3,4 The two most common forms of EGFR mutations are exon 19 deletions and the Leu858Arg mutation (L858R), comprising 45% and 40% of NSCLC cases respectively.5 Studies examining the biological and clinical characteristics of these mutations have shown a greater prevalence in females, never-smokers, and individuals of Asian ancestry.6,7 Radiologically, these mutations are associated with pure or mixed ground-glass opacities in CT, as well as longer volume-doubling times, implying a slower growth rate.8,9 This is consistent with studies demonstrating a better prognosis for patients with EGFR mutations versus those without it,10–14 which may be attributable to advancements in novel therapies, including EGFR tyrosine kinase inhibitors (EGFR-TKIs).
The correlation between EGFR mutation and response to targeted treatment was first reported in 2004.15–17 Subsequent studies have demonstrated improved survival, and quality of life for patients treated with these targeted agents.18–20 Although first line treatment for early stage lung adenocarcinoma is surgical resection or stereotactic radiation, approximately 70% of NSCLC cases are diagnosed with unresectable disease,21 highlighting the need for systemic therapies. One available option is erlotinib, an EGFR-TKI that has been shown in three randomized controlled trials (RCTs) to improve progression free survival (PFS) by 4.5 months compared to conventional chemotherapy.22–24 By one estimate, the 5-year survival among EGFR-mutant metastatic lung adenocarcinoma patients treated with erlotinib or gefitinib is 14.6%.25 Although better tolerated than traditional chemotherapies, EGFR-TKIs can cause severe adverse events (AEs), such as cutaneous reactions, paronychia, and intolerable diarrhea.26
Here we describe the case of a woman who was diagnosed with locally metastatic NSCLC, and distinct pulmonary masses, later identified as two independent primary lung tumors based on genetic profile. To the best of our knowledge, no other such reports in which testing for these driver mutations helped establish a diagnosis of concomitant NSCLCs in a single patient.
Case Report
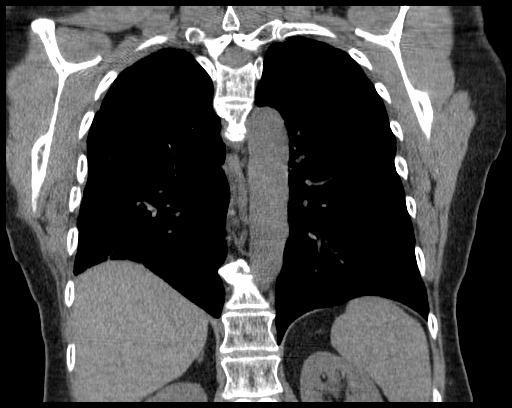
A 58-year-old-female, never-smoker, without a family history of cancer, presented to her primary care physician with several weeks of cough and blood-tinged sputum five years ago. A CT-chest showed a 4.3cm mass in the right lung apex, a 2.0 cm nodule in the RLL with several small indeterminate nodules, along with right paratracheal and hilar adenopathy. A subsequent PET-CT scan showed intense uptake in the right upper (SUV 12.2) lobe (RUL) and right lower (SUV 2.5) lobe (RLL) masses, and in the mediastinal lymph nodes, but no extra-thoracic sites of disease were detected (Figure 1, A&C). A brain MRI was negative for disease, and she was staged IIIB. She was taken for bronchoscopy and underwent fine needle aspiration (FNA) of a 4R lymph node as well as a broncho-alveolar lavage (BAL) of the RLL lesion. This confirmed the presence of poorly differentiated adenocarcinoma. Pathology was sent for PCR analysis (PhenoPath Laboratories, Seattle WA) and was found to be positive for the L858R EGFR mutation. After discussion at multidisciplinary tumor board conference, the question was raised of whether the RUL lesion was a primary vs secondary malignancy. She was then taken for EMN biopsy of both RUL and RLL lesions, both were positive for adenocarcinoma. PCR testing were sent separately for both samples and the RLL was positive for exon 19 deletion and the RUL was positive for L858R mutation. Neither tumor was positive for the T790M mutation.

Two months later, she was started on systemic therapy with erlotinib. She developed a diffuse red and pustular raised rash on her face and much of her body, as well as several small mouth sores, with a brief episode of epistaxis that resolved spontaneously. Despite this, she felt well enough and wanted to continue therapy. Repeat PET-CT four months later showed CR in the RLL, and PR in the RUL (Figure 1, B&D). The decision was made to pursue aggressive surgical intervention with RUL/RLL bilobectomy a month later. Pathology showed evidence of N2 disease; therefore, at time of surgery she was stage IIIA, presumably of the RUL mass, with mediastinal lymph node involvement. The RLL mass was presumed to be stage I (versus stage IIA). These were successfully resected, and she was subsequently deemed to have NED (Figure 2).

As per standard of care, adjuvant cytotoxic chemotherapy was pursued with curative intent using cisplatin/premetrexed starting October, 2017—one month after her bilobectomy. She completed four-cycles, ending within three months. Given her impressive response to anti-EGFR therapy previously, but no clear previously published guidelines for therapy at this point (she was NED), the decision was made to re-initiate erlotinib at 150mg daily for 2 years per the ALCHEMIST trial.27 This was started five months later and she again experienced dermatitis with a new episode of Methicillin Sensitive Staphylococcus Aureus (MSSA) cellulitis seven months later. Additionally, she experienced difficulties with cognition and emotionality. Although mild at first and attributed to concomitant adjustments being made to her thyroid medications, the symptoms continued throughout her treatment course.
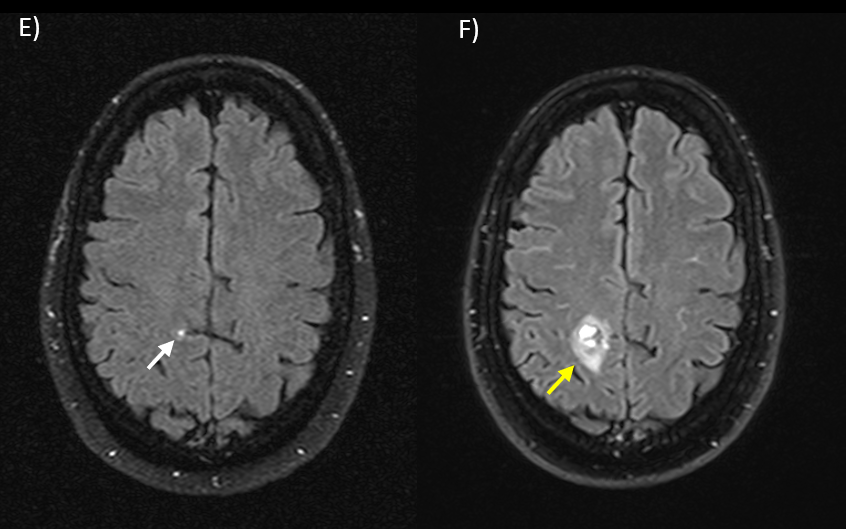
Screening CT scans were performed every three months, which showed NED. A brain MRI five months after erlotinib resumption unfortunately showed a new ill-defined 5 mm enhancing and FLAIR hyperintense focus in the right parietal lobe cortex, suspicious for metastasis. This new brain mass remained stable on imaging until nine months later where an interval increase in size to 1.5cm was noted (Figure 3), along with internal necrosis, hemorrhage and surrounding vasogenic edema. In consultation with the Radiation Oncology team, a decision was made for Stereotactic Radiosurgery (SRS) treatment. She tolerated SRS at 2700 cGy over three fractions without any adverse central nervous system (CNS) side effects. An MRI two months later showed interval decrease in size of parietal lobe lesion, which remained stable on follow up imaging. In terms of her persistent cognitive difficulties, she was seen by Neurology and dexamethasone was started for question of leptomeningeal disease given subtle FLAIR changes seen on MRI. She had symptomatic improvement but was unable to taper below 2mg/daily. Consequently, a diagnostic lumbar puncture (LP) was performed three months later which revealed infiltration by lung adenocarcinoma. The decision was made to start Osimertinib for better cerebrospinal fluid (CSF) penetration. This resulted in persistent improvement in clinical symptoms and shrinkage of lesions on MRI.

Discussion
Although co-mutations within the same tumor have been reported in up to 12% of NSCLC patients,28 we are not aware of other cases in which a single patient was diagnosed with two separate primary lung tumors based on genetic profiles. There is evidence that different EGFR mutations represent distinct disease entities that respond differently to treatment with specific TKIs.29 The response rate to first-line treatment with EGFR TKIs across all mutations approaches 70%, comparing favorably with a 30% response rate to first-line chemotherapy.30
This patient underwent neoadjuvant erlotinib followed by surgical resection and adjuvant cisplatin doublet therapy, which has been shown to improve overall survival (OS) by 4-15% in patients with stage I-III NSCLC.31–33 She was then restarted on erlotinib, and remained NED until one year later when a brain MRI noted a 5mm lesion concerning for metastasis. Her 17 months progression free survival (PFS) is similar to the reported median of 10 to 16 months34 among patients with single gene mutations undergoing EGFR-TKI therapy. This is also in line with studies showing that certain co-mutations portend a poorer prognosis while others do not clearly have this effect. For example, coincidental mutations in non-driver genes such as tumor protein p53 gene (TP53) are relatively high (>5%) in the EGFR-mutated population and are associated with higher tumor grade and shorter PFS/OS during EGFR TKI therapy.35,36 It should be noted that our patient tested negative for the TP53 mutation.
Some studies indicate that co-mutation may be associated with higher rates of primary resistance to TKIs.37,38 However, the most frequent cause of secondary resistance to these agents is acquisition of a novel resistant mutation which is most often the T790M mutation, present in approximately 50% of cases.39 Progress has been made in overcoming secondary resistance in patients with the T790M mutation by using third-generation EGFR TKIs, such as Osimertinib. Recent results form the ADAURA clinical trial have also shown that adjuvant use of Osimertinib resulted in improved disease free survival (DFS) in patients with EGFR-mutated lung adenocarcinoma, and this has now become the new standard of care.40 In our patient’s case, a clinical response to Osimertinib has been maintained. However, she remains at risk for further progression, at which point next-generation sequencing (NGS) will likely be performed to establish her molecular signature and determine candidacy for further targeted therapy.
There continue to be rapid advances focused on overcoming resistance to third-generation TKIs including the use of combination therapies, antibody–drug conjugates, bispecific antibodies, and even the development of fourth-generation TKIs. We hope that such treatment modalities will be able to provide meaningful and prolonged clinical improvements for patients similar to the one described in this case.
Conflict of Interest
None
Funding information
None
Ethical statements
This research was conducted in accordance with the principles outlined in the Declaration of Helsinki. Our institution does not require IRB approval for case reports.
Acknowledgement
N/A
Author contributions
i. Junid Naveed Ahmad: conception and design
ii. Bowen He: data collection and assembly
iii. Junid Naveed Ahmad: data analysis, manuscript writing
iv. Brett Schroeder and Joseph Rosales: manuscript review
All authors have approved the manuscript