
Introduction
The COVID-19 pandemic resulted in many adverse effects on health outcomes. At the start of the pandemic, United States (US) healthcare facilities limited “non-essential” services in preparation for an influx of patients ill secondary to SARS-CoV2 infection. This led to significant reductions in nonurgent clinic visits with an estimated 60% decline in all ambulatory visits, including cancer screenings in April 2020.1,2 Cancer screenings are imperative for early detection, which can impact prognosis.3 Recent data demonstrates breast, colorectal, and prostate cancer screenings declined between March and May of 2020 compared to the same time period in 2019, with the sharpest decline in April (breast -90.8%, colorectal -79.3%, and prostate -63.4%).1 This decline and the potential downstream consequences are concerning. A recent study has predicted in excess of 10,000 deaths from breast and colorectal cancers in the next decade,4 possibly from stage migration or patients presenting at more advanced stages due to missed screening.
The COVID-19 pandemic has also highlighted the stark inequities ingrained in the US healthcare system, which disproportionately impact communities of color. These inequities also contribute to the disparate cancer-specific outcomes of minority populations in the US. In general, ethnic/racial minorities have lower access to high-quality cancer care and present with more advanced disease at diagnosis compared to non-Hispanic Whites.5,6 In breast cancer, Black, American Indian, and Hispanic/Latina women have higher risk of breast cancer-specific mortality relative to White women.7 Black men and women also have the highest rates of colorectal cancer of any ethnic/racial group in the US. Mortality rates from colorectal cancer are 47% higher in non-Hispanic Black men and 34% higher in non-Hispanic Black women compared to White men/women.8 In prostate cancer, Black men have 1.8 times higher incidence and 2.2 times the rate of mortality compared to White men.8 These inequities may be further widened in the context of reduced cancer screening activities.
In this study, we used electronic health record (EHR) data from the Reliable Response Data Discovery for COVID-19 (R2D2) research team consortium9 to evaluate the ethnic and racial differences in breast, colorectal, and prostate cancer screening and diagnosis during the COVID-19 pandemic. We hypothesized that there would be a difference based on ethnicity and race with regards to how the COVID-19 pandemic disrupted cancer screening surveillance and diagnosis.
Methods
Study Design
We conducted an analysis of EHR data from 8 health systems (in appendix) supported by the R2D2 research network.9 IRB approval was obtained at each site. R2D2 is a consortium of institutions and investigators that support the use of EHR data from their health systems in the Observational Medical Outcomes Partnership (OMOP) Common Data Model.10 OMOP data marts supported at each institution can be analyzed using a common structured query language (SQL) query, and R2D2 facilitates structuring, distributing, and troubleshooting queries, and then concatenating results from each health system into a single dataset of aggregated results (blinded to health system).11,12
Key Procedure/Outcomes
We constructed a set of queries that derived a monthly count for different types of medical procedures and diagnoses related to screening, diagnosis, and treatment of breast, colon, and prostate cancer, between January 2019 and January 2021. Code lists used for each query are provided in the appendix and were aligned for all sites. Counts were the number of unique patients who received at least one of each procedure/diagnosis type each month, at each health system by race (American Indian or Alaskan Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, Other Race, Unknown), ethnicity (Hispanic or Latino), and sex (Female, Male) as recorded in each EHR system.
Population Selection
The population for the study was identified by the number of individuals that had the procedure of interest during the study period. This was used as the baseline numerator, with the assumption that the number of eligible patients is stable over time.
Statistical analysis
Descriptive statistics were used to summarize the encounters including disease type, race, and ethnicity. Individuals for whom race or ethnicity data were missing were excluded from the final analysis as our objective was to characterize screening for each ethnic/racial group. The relative percent change in screenings, diagnosis, and treatment was calculated from pre-pandemic baseline levels (average rates taken from January 2019 to February 2020) to each month between January 2019 and January 2021. Distributions of race and Hispanic ethnicity in the pre-pandemic era were compared to April 2020 and July 2020, separately, using a Chi-squared test using SAS 9.4.
The weekly COVID incidence rate at the national level was also obtained and compared with screening events for breast, colon, and prostate cancer screenings.
Results
General Characteristics
A total of 2,878,967 events (patients of a given race, ethnicity, or sex with a given procedure in a given month) were extracted. A subset of 386,409 lacked ethnicity/race data and therefore were excluded from analysis. This proportion of missing data remained largely constant during the study period. Among evaluable events, 1,060,308 (43%) were for breast cancer, 536,297 (22%) for colon cancer, and 1,282,362 (51%) for prostate cancer. The characteristics of these events are summarized by disease type and ethnic/racial groups in Table 1.

Breast Cancer
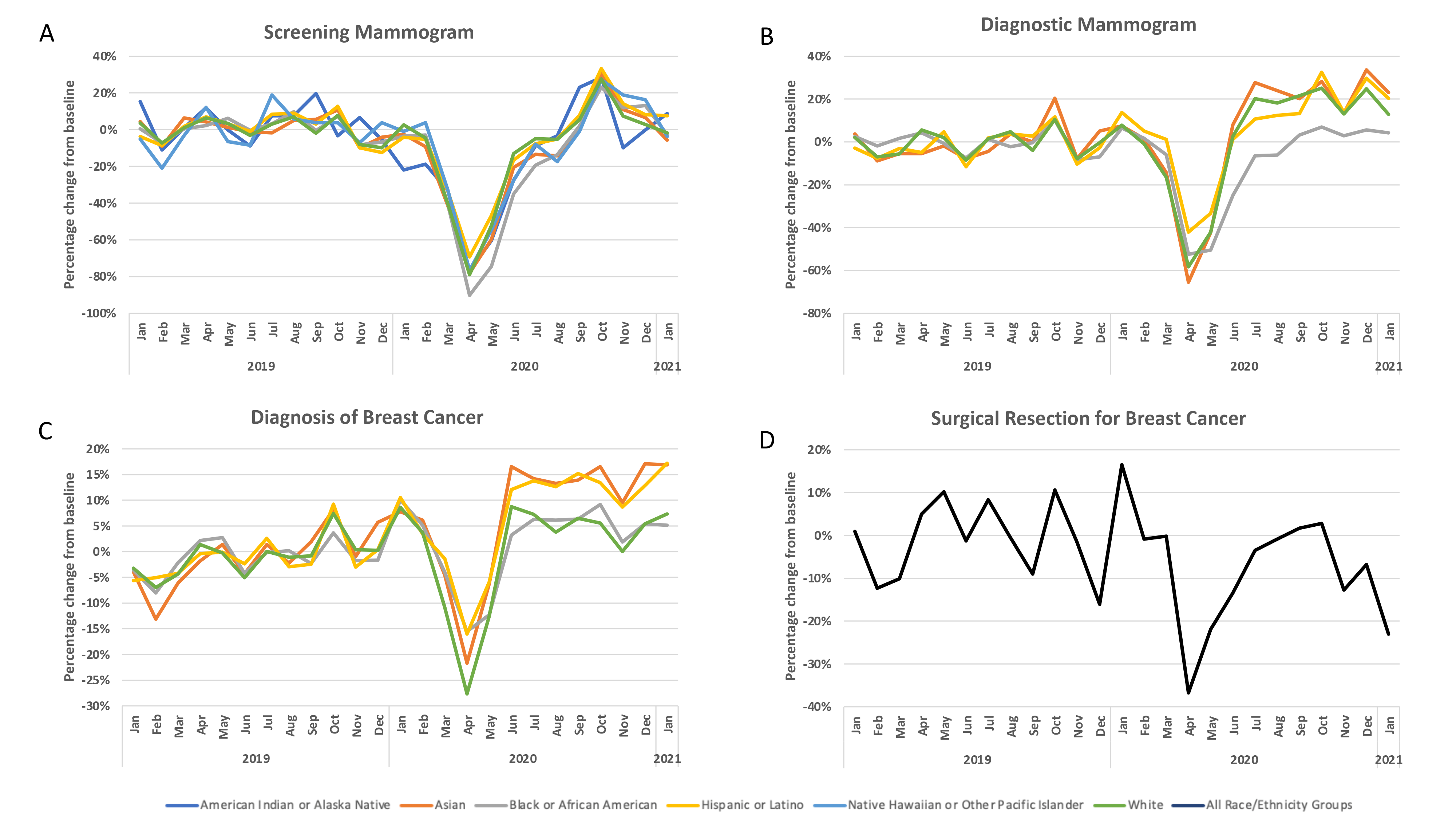
A significant reduction in screening mammography was observed for all groups between March and May of 2020, with the largest relative decline in April (Figure 1a) during the initial SARS-CoV2 surge. In that month, there was a relative reduction in screening mammography by 90% for Black, 79% for White, 78% for Asian, and 69% for Hispanic individuals. The absolute number of American Indian/Alaskan Native (AI/AN) and Native Hawaiian/Pacific Islander (NH/PI) groups was very small, but we observed similar patterns of reduction by 77% for both groups. For White individuals, screening mammograms largely returned to pre-pandemic baseline by July of 2020. However, a further lag was observed for all other groups until September of 2020. Racial and Hispanic ethnicity distributions were calculated in April 2020 and July 2020 and compared to the pre-pandemic baseline (Table 2). We observed a higher proportion of White, Asian, and Hispanic individuals, and much lower proportions of Black individuals receiving screening mammography in April 2020 compared to pre-pandemic baseline (White 76% vs 69%; Asian 14% vs 12%; Hispanic 18% vs 12%, Black 9% vs 18%; p<0.0001). By July 2020, the racial distributions were more like pre-pandemic levels, but still statistically significantly different (White 72%; Asian 11%; Black 16%; p<0.0001); whereas the proportion of Hispanic was the same (12%; p=0.66).

A reduction in diagnostic mammography was also observed for all groups between March and May of 2020, with the largest relative decline in April (Figure 1b) during the initial SARS-CoV2 surge. In that month, there was a relative reduction in diagnostic mammography by 66% for Asian, 58% for White, 52% for Black, and 42% for Hispanic. There was a higher proportion of Black (26% vs 23%; p=0.018) and Hispanic (16% vs 12%; p<0.0001) individuals, and lower proportions of Asian and White individuals (White 66% vs 67%; Asian 8% vs 10%; p=0.018) receiving diagnostic mammography in April 2020. By July 2020, the racial distributions remained different with higher proportions of White and Asian and lower proportions of Black individuals receiving diagnostic mammography (White 71%; Asian 11%; Black 19%; p<0.0001); whereas the proportion for Hispanic was the same (12%; p=0.58).
We also noted a change in the racial distribution of breast cancer diagnoses, with higher proportions of Hispanic (10% vs 9%; p=0.004), Asian (12% vs 11%; p=0.0009), Black (11% vs 9%; p=0.0009) individuals and lower proportions of White (78% vs 79%; p=0.0009) individuals being diagnosed with breast cancer in April 2020 compared to pre-pandemic baseline. By July 2020, the racial and ethnic distributions in breast cancer diagnoses were more like pre-pandemic levels (White 79%; Asian 12%; Black 9%; p=0.25); and Hispanic (9%; p=0.21). However, we note a relative increase in breast cancer diagnoses in Asians and Hispanics after June 2020, with an average of 8% and 13% increased events respectively (Figure 1c).
Surgical resections for breast cancer across all groups were reduced by up to 37% in April of 2020 (Figure 1d) during the initial SARS-CoV2 surge. This returned to the pre-pandemic baseline by August/September of 2020. However, by October of 2020, surgical resections started to decrease again coinciding with the start of the third SARS-CoV2 surge. On average surgical resections for breast cancer were 7% lower between June 2020 and January 2021 compared to the pre-pandemic baseline.
Colon Cancer
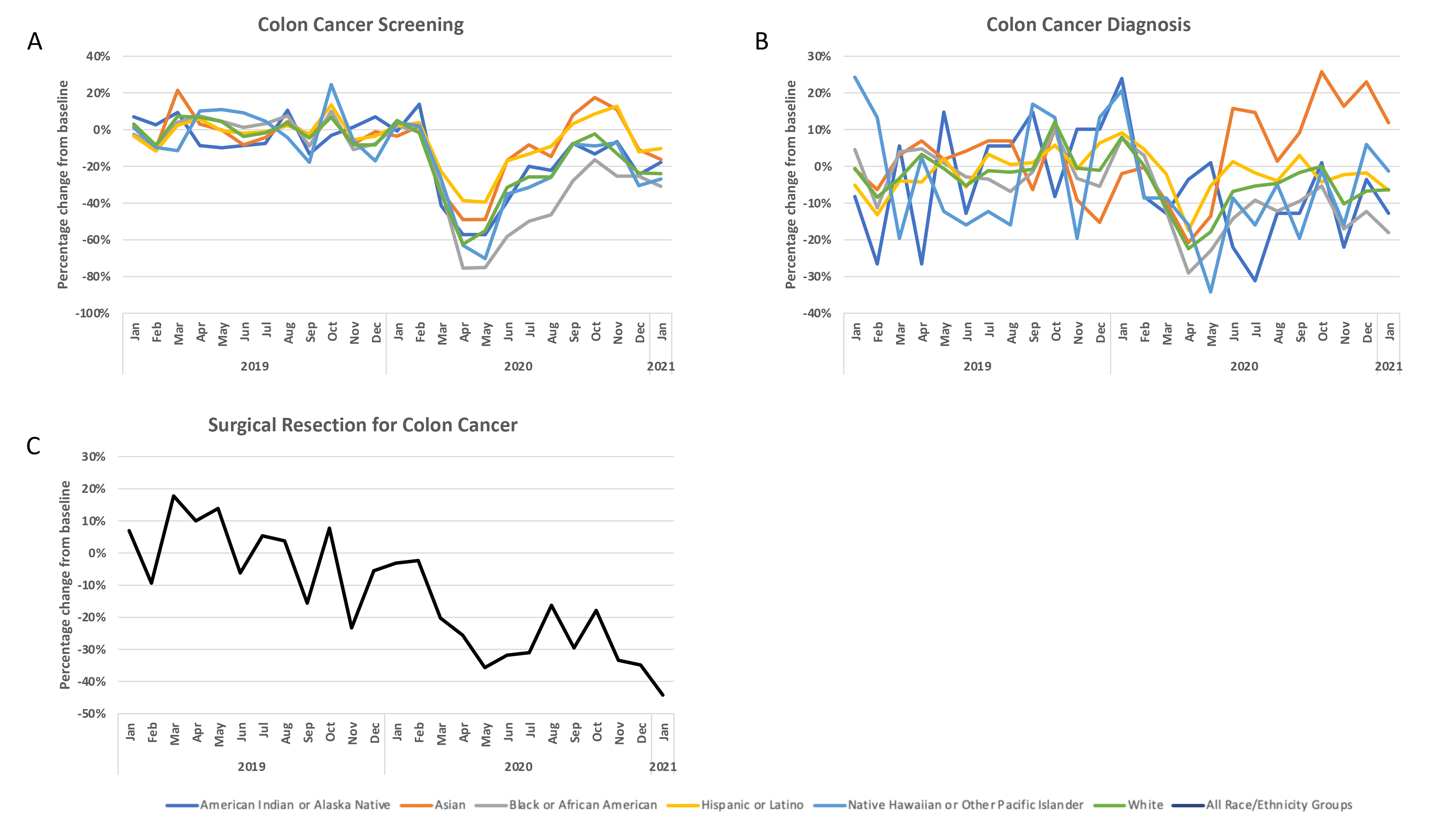
There was a reduction in colon cancer screening for all groups between March and May of 2020, with the largest relative decline in April (Figure 2a) during the initial SARS-CoV2 surge. In that month, there was a relative reduction in colon cancer screening by 75% for Black, 62% for White, 49% for Asian, and 39% for Hispanic. The absolute number of AI/AN and NH/PI groups was very small, but we observed similar patterns of reduction in colon cancer screening by 63% for NH/PI and 57% for AI/AN. These counts returned to the pre-pandemic baseline by September of 2020 for Asians, but not for any other ethnic/racial group. The largest reduction was for Black individuals who had an average of 35% reduction in colon cancer screening between June 2020 and January 2021. We also observed a change in the racial distribution, with higher proportions of Asian and White individuals and lower proportions of Black individuals receiving colon cancer screening in April 2020 compared to the pre-pandemic baseline (White 75% vs 74%; Asian 13% vs 9%; Black 11% vs 16%; p<0.0001). The proportion of Hispanic individuals getting colon cancer screening was also higher in April 2020 (18% vs 12%; p<0.0001). By July 2020, the racial distributions were more like pre-pandemic baseline but remained statistically different (White 76%; Asian 12%; Black 11% p<0.0001); the proportion of Hispanic individuals was also different (14%; p<0.0001).

The absolute colon cancer diagnoses were small in this dataset and racial distributions were not statistically different in April 2020 or July 2020 compared to baseline. There is a trend toward higher counts of colon cancer diagnoses in Asian individuals between June 2020 and January 2021 (Figure 2b). However, the total events for these individuals were small, and the trends were unstable.
The aggregated counts of surgical resection for colon cancers show an overall decreasing trend, especially during the first and third SARS-CoV2 surges, with an average of 30% reduction in surgical resections for colon cancer between June 2020 and January 2021 (Figure 2c).
Prostate Cancer
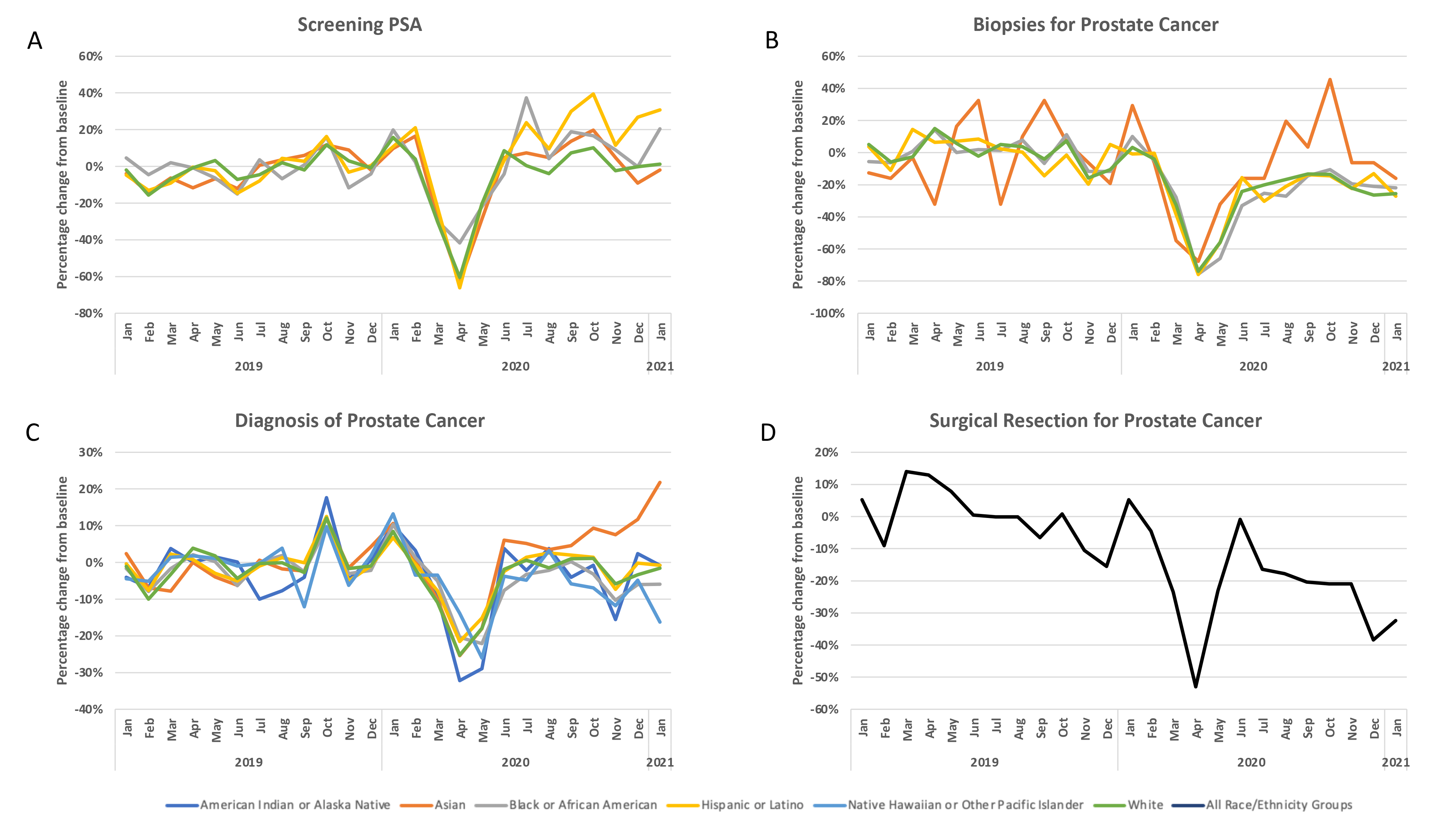
There was a reduction in prostate cancer screening via serum prostate-specific antigen (PSA) test for all groups between March and May of 2020, with the largest relative decline in April (Figure 3a) during the initial SARS-CoV2 surge. In that month, there was a relative reduction in PSA screening by 66% for Hispanic, 63% for Asian, 60% for White, and 42% for Black. We also observed a change in the racial distribution, with higher proportions of Black individuals, and lower proportions of White and Asian individuals receiving PSA screening in April 2020 compared to the pre-pandemic baseline (Black 9% vs 6%; White 82% vs 84%; Asian 9% vs 10%; p<0.006). The proportion of Hispanic individuals getting PSA screening was not statistically different in April 2020 compared to the pre-pandemic baseline (7% vs 8%; p=0.16). By July 2020, the racial distributions remained different (White 81%; Asian 11%; Black 8%; p<0.007 and the proportion of Hispanic individuals increased (9%; p=0.027) compared to the pre-pandemic baseline.

Diagnostic biopsies obtained for prostate cancer were also reduced for Black, White, and Hispanic individuals (Figure 3b). However, the racial and ethnic distribution in April/July 2020 did not differ significantly from the baseline (Table 2). This reduction did not return to the pre-pandemic baseline for all groups, with an average relative reduction of 22% for Black and 20% for White and Hispanic individuals.
There was a reduction in prostate cancer diagnoses for all groups during the initial SARS-CoV2 surge, between March and May of 2020. In April 2020, we observed a change in the racial distribution, with a higher proportion of Black individuals, and a lower proportion of White individuals diagnosed with prostate cancer compared to the pre-pandemic baseline (White 67% vs 69%; Black 30% vs 28%; p=0.001). The proportion of Hispanic individuals diagnosed with prostate cancer in April 2020 was not different compared to baseline (6%; p=0.35). By July 2020, the racial (p=0.10) and ethnic (p=0.53) distributions were similar to baseline.
Surgical resections for prostate cancer across all groups were small and unstable but showed a general decreasing trend, especially during the first and third SARS-CoV2 surges. The total number of resections remained lower than the pre-pandemic baseline, with an average of 21% relative reduction between June 2020 and January 2021.
COVID-19 Effect on Cancer Screening
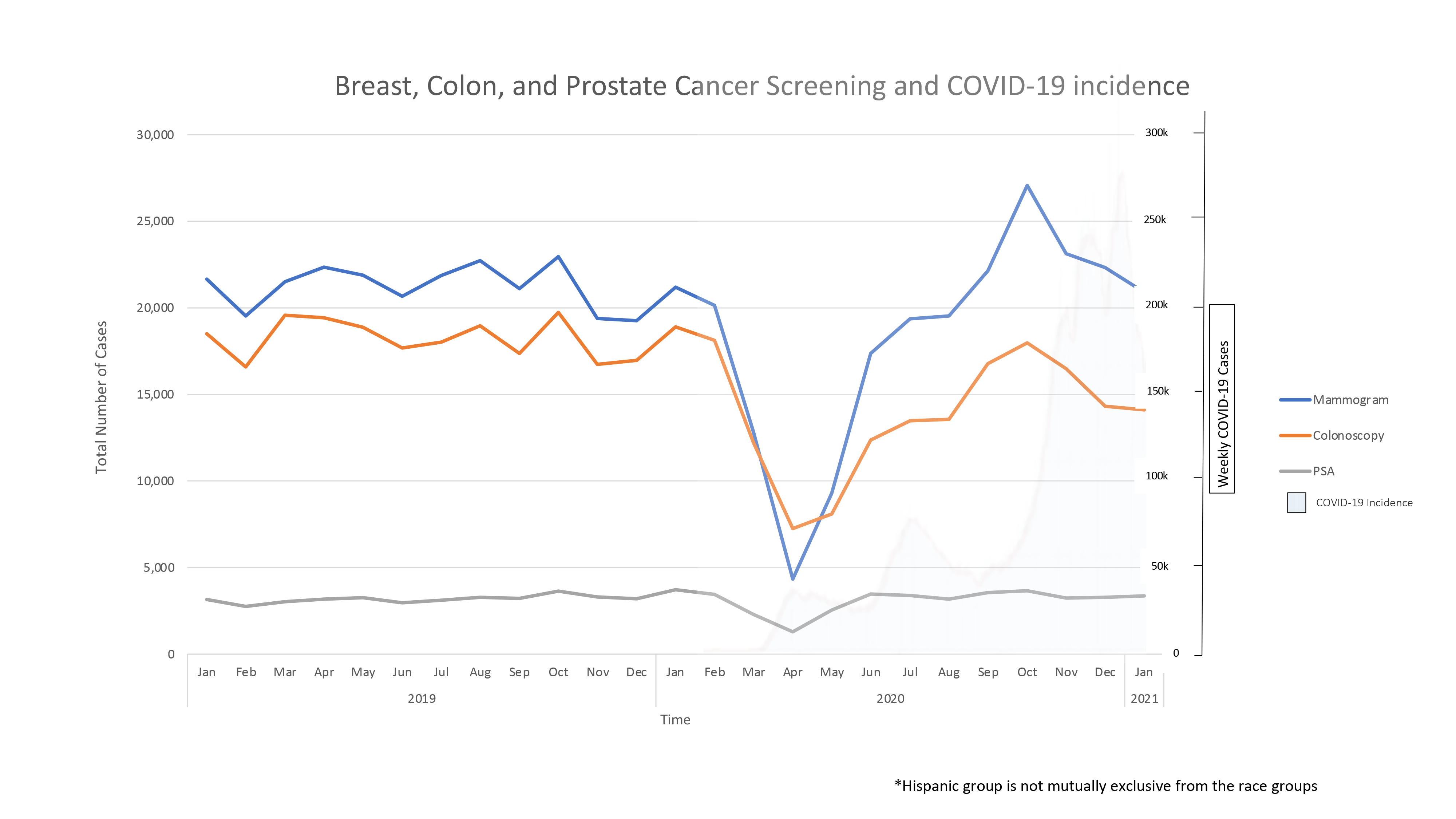
The largest reduction in screening for breast, colon, and prostate cancers occurred between March and May of 2020 coinciding with the first surge of the COVID-19 infections and after many states instituted “Shelter in Place” orders. Figure 4 illustrates the screening rates for breast, colon, and prostate cancer superimposed with the weekly infection trends in the US reported to the Centers for Disease Control (CDC).13 This demonstrates there is another small reduction with the third wave of COVID-19 infection for screening mammography and colon cancer screening, but not for PSA screening. A reduction in cancer screenings was not associated with the second surge of COVID 19 infections.

Discussion
Differential inequities in cancer screening and diagnoses were observed by race and ethnicity and corresponded primarily to the initial surge of SARS-CoV2. Although Black women have the highest breast cancer-specific mortality rate of all ethnic/racial groups, they had the highest relative reduction in breast cancer screening. They also had delayed return to pre-pandemic screening rates compared to their White counterparts, consistent with findings from other groups.14–16 We expect the effects of this delayed screening to exacerbate the existing breast cancer disparities for Black women. Modeling studies from the National Cancer Institute (NCI) have already predicted increased cumulative excess breast cancer deaths related to due to pandemic-related disruptions, including screening.17 It has also been previously established that less frequent mammographic screening can be associated with greater frequency of more advanced-stage disease and development of interval cancers,18 which can be associated with more aggressive features.19 Therefore, it is imperative that we make up for these missed screening mammograms in the coming months.
The relative increase in diagnostic mammograms observed for all ethnic/racial groups other than Black ethnicity after June 2020, may be alluding to possible stage migration as symptomatic patients present to medical attention. We note the limitation in our dataset in that we cannot ascertain which of these diagnostic mammograms are new evaluations versus follow-up examinations from prior abnormal mammograms. The marked reduction in breast cancer diagnoses seen between March and May of 2020 is likely an effect of decreased screening and ambulatory care rather than a true reduction in breast cancer incidence. The change in the distribution of breast cancer diagnoses in April of 2020 as compared to July 2020 was likely confounded by the change in the rates of screening mammograms during this period. We noted an increased number of breast cancer diagnoses for Asian and Hispanic individuals between June 2020 and January 2021, though we cannot conclude from this data set whether this is a true increase in incidence given the numerator-only nature of our analysis. We also acknowledge the limitation of ICD-10 code use, which cannot ascertain the stage to confirm stage migration.
Our data also demonstrates reductions in colon cancer screening for all groups and the persistence of this decline throughout the rest of 2020, with the largest reduction in Black individuals, who in general have the highest colon cancer-related mortality of any ethnic/racial group. The distributions of colon cancer screening encounters (by ICD10 codes) are likely affected by the overall reduction in colon cancer screenings (especially procedural ones such as colonoscopies). A major limitation in our analysis is that we were not able to stratify which colon cancer screenings are noninvasive (fecal occult blood or DNA-based tests) as compared to invasive ones, such as colonoscopies. Regardless, our findings of a marked reduction in colon cancer screening in Black individuals are consistent with findings from other institutions across the US.20,21 The implications of this trend are alarming as the population which bears the greatest burden of colon cancer-related mortality8 is also one that has had the largest reduction in screening associated with COVID 19 pandemic.
Interestingly, there was a relative increase in colon cancer screening for Asians after July 2020 and an associated increase in colon cancer diagnoses during the same time. Historically, all Asian subgroups other than Japanese and US-born Chinese have lower colorectal cancer incidence compared to the non-Hispanic White population.22 This increase in colon cancer diagnoses may be related to the increased screening rates in this population. However, more data is needed to assess the significance of this finding.
Annually there are about 104, 270 cases of new colon cancer in the US. About 38% of these tend to be ones diagnosed at an early stage.23 Assuming our data is representative of the US population, the average of 30% reduction in colon cancer surgical resections in 2020 may result in delayed curative treatments for at least 11,887 patients with early-stage colon cancer.
Prostate cancer screening seems to have been affected the least by the COVID-19 pandemic. This is likely due to the non-invasive nature of PSA screenings. A limitation of our data source is that it does not differentiate which PSA examinations are new versus follow-up evaluations. Furthermore, we observed that surgical resections for prostate cancer did not return to the pre-pandemic baseline, with about a 21% relative reduction. In general, prostate cancer surgery24,25 and biopsies26 have been decreasing over time due to concerns regarding overtreatment. Therefore, this observation may not be solely attributable to COVID 19 pandemic.
Conclusion
Overall, our study uses large data across diverse clinical sites. Six out of the eight institutions which provided this data were in California, which may introduce some bias, though the Veterans Affairs (VA) system provides national data. Other limitations of our study include missing data for ethnicity and/or race for 13% of events, which were omitted from the final analysis. Missing data for ethnicity/race may be biased towards people of color and thus the inequities we have described here may be affected. In addition, there were few events representing AI/AN and NH/PI groups, therefore we were unable to always analyze that subset of our data.
We have demonstrated that the reduction in cancer screening for breast, colon, and prostate cancer during 2020 did not always correlate with surges in SARS-CoV2 infections. This was likely due to the rapid shift of non-urgent ambulatory visits to telehealth visits and the decrease in non-urgent invasive and noninvasive procedures early in the pandemic. As new variants of the SARS-CoV2 emerge, it is imperative that health systems continue cancer screening, along with strengthening safeguards to limit contagion. Robust information systems need to be maintained to ensure the importance of cancer screenings continues in an era of misinformation. Increasing access to cancer screenings equitably in the coming years remains crucial to make up for the “missed screenings” of early 2020 and minimize the risk of widening existing cancer disparities.
Conflict of Interest
None
Funding information
This study was supported in part by the NIH National Cender for Advancing Translational Science (NCATS) through the UCLA CTSI, Gant Number UL1TR001881.
HTB is funded by the Prostate Cancer Foundation
Ethical statements
N/A
Acknowledgments
N/A
Author contribution
i. Dame Idossa, Hala T Borno, Gillian Gresham: conception and design
ii. Dame Idossa, Hala T Borno, Gillian Gresham, Katarina Wang: data collection and assembly and manuscript writing.
iii. Alison J. Canchola, Lucila Ohno-Machado, Mark Pletcher,Jihoon Kim, : data analysis, manuscript writing.
All authors have approved the manuscript.