



INTRODUCTION
Head and neck cancer is prevalent in developing countries, particularly in rural communities, due to the use of tobacco, tobacco-related products and alcohol.1–4 The treatment of head and neck cancer in a rural setting is usually complex and not considered feasible. Delivering oncologically specific treatment that involves multimodality management (surgery, chemotherapy, radiotherapy), particularly in a resource-constrained community, is a significant challenge.5 Several factors impact the possibility of the treatment, including the inadequacy of infrastructure, treatment standardization, finances, logistics and technical limitations, all of which had profound impact the outcome. Moreover, patients in a rural setting usually present with advanced stage, thus making it very crucial to start treatment on time.3,6–8 It turns out to be very problematic for patients to receive appropriate treatment due to the gross scarcity of decentralized cancer centers in Nepal. Prevailing public perception that the tertiary care model in rural settings provides sub-optimal care is a barrier that is hard to overcome, consequently leading to fewer people seeking care in our hospital.
According to GLOBOCAN 2020, oral cancer is the eight most common cancer in the world among men.9 Cancers of the lip and oral cavity are widespread in Southern Central Asia and it is also the leading cause of cancer death in India among men.1–4,10–12 More than 60% of oral cancers in South Asian countries are still diagnosed in locally advanced stages.3,6,7,13 Eighty percent of oral cancers occur in patients with low socio-economic status who are likely tobacco users and live in areas without standard facilities for treating oral cancers.3,7,8,11,13,14 Five-year survival among head and neck cancer patients in developed countries ranged between 0.3% and 12.6%, whereas in developing countries, it ranged between 1% and 4.7%.15 Lip and oral cavity cancer account for 10.2 per 100,000 in lower Human Development Index (HDI) countries because of the high burden of the disease in India.9
The Global Cancer Observatory 2018 estimated the age-standardized cancer incidence and mortality rates in Nepal to be 103.7/100,000 and 77.8/100,000, respectively.10–12 In Nepal, approximately 27000 new cancer cases /year are detected and, the prevalence is twice as new cases.11,12,16 In Nepal, cancer accounted for 10% of total deaths, and oral cavity cancer was the fourth most common cause of death from cancer among males in the year 2017.11,12,16 In one of the recent studies from Nepal, oral cancer accounted for second highest prevalent cancer amongst men and third most prevalent cancer amid women.11 In an analysis report of cancer burden in Nepal, lip and oral cavity cancers accounted for 5.19% (N=1426) of the total cancer cases in the year 2015.12 In Madhesh province of Nepal, where the total population is 6,126,288, the number of cancer cases reported was 1210 accounting for 12.5% of total cancer cases of Nepal in 2015.11,12,16 According to Population Based Cancer Registry of Nepal, oral cancer is the leading cause of cancer among men in Dhanusa district with Age-Adjusted Rate of 6.62 per 100000 population in 2018.17 This region (Madhesh province) is highly exposed to the use of tobacco and tobacco products consumption resulting in a higher incidence of oral cancers and no head and neck oncology programs have yet been implemented in this region. A tertiary cancer center (BTFCC), located in Janakpur city of Dhanusa district of Madhesh province has established head and neck oncology department to address these issues and provide multimodality cancer care in rural Nepal. We aim to share our experiences delivering services to the rural community.
METHODS
Research design
This descriptive retrospective study includes the data of all patients who visited the Head and Neck Surgical Oncology department at the tertiary cancer center (BTFCC), Janakpur, Nepal between April 2022 to December 2022, with a lesion suspicious of oral cancer. Data was extracted from the Electronic Medical Record system of the hospital by the head and neck cancer specialist, who is also the author of this article. In addition, this study utilized several sources of secondary data.
Data analysis
Patient data was stratified as per the statistical necessity and all statistical analyses were done using Statistical Package for Social Sciences (SPSS) 25 software from IBM® Corp. The data is tabulated and descriptive analysis is represented in graphical forms to summarize, organize, evaluate, and interpret the numeric information. The uniformly collected data includes:
-
Demographics- Age, gender and occupation distribution of patients
-
Clinical Findings- Distribution of patients according to diagnosis, differentiation of oral cancer and Oral Potentially Malignant Disorders (OPMD), and prior history of tobacco intake. The presentation stage, site and recommended treatment plan were also analyzed in patients with oral cancers.
RESULTS
Demographic Findings
The average age of presentation was 47.20±2.9 years with the range of 21-75 years of age. (Fig 1) The most frequent age group presentation was 30- 39 years followed by 60-69 years.

Of the total 30 patients, 21 (70%) were male and rest nine (30%) were females, with a male-to-female ratio of 2.3:1. The prevalence of oral cancer was more in males (86.7%, N=13) than in females (13.3%, N=2). Similarly, the prevalence of oral cancer and OPMD was higher in males (76.19%, N=16) than in females (23.81%, N=6). The patients were also grouped based on occupation into nine groups and their frequency seen were Driver (3.3%, N=1), Unemployed (23.3%, N=7), Homemaker (36.7%, N=11), Laborer (10%, N=3), Farmer (3.3%, N=1), Doctor (3.3%, N=1), Student (6.7%, N=2), Businessman(10%, N=3) and Social worker (3.3%, N=1).
Clinical Findings
We recorded various spheres of clinical findings and recommended treatment.
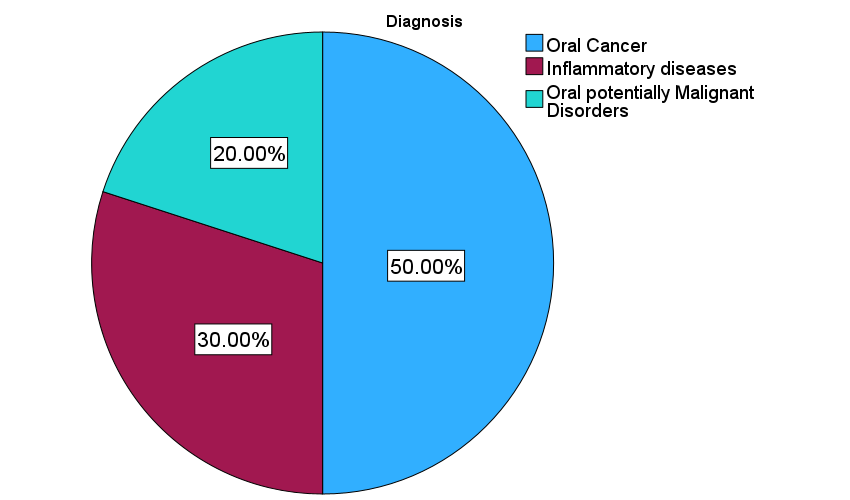
Oral cancer was diagnosed in 50% (N=15), OPMDs in 20% (N=6) and other inflammatory diseases in 30% (N=9) of the total patients. (Fig 2)

The median time duration of visit to our hospital by the patients after noticing initial disease symptoms was 3.50 months with a range of 1 to 120 months. (Fig 3)

Among oral cancer, 86.7% (N=13) were diagnosed as squamous cell carcinoma, 6.7% (N=1) as squamous cell carcinoma-in-situ and 6.7% (N=1) as verrucous carcinoma. (Table 1)
Among OPMDs, 66.6% (N=4) were oral submucous fibrosis, 16.7% (N=1) were candidiasis and 16.7% (N=1) were morsicatio buccarum. (Table 2)
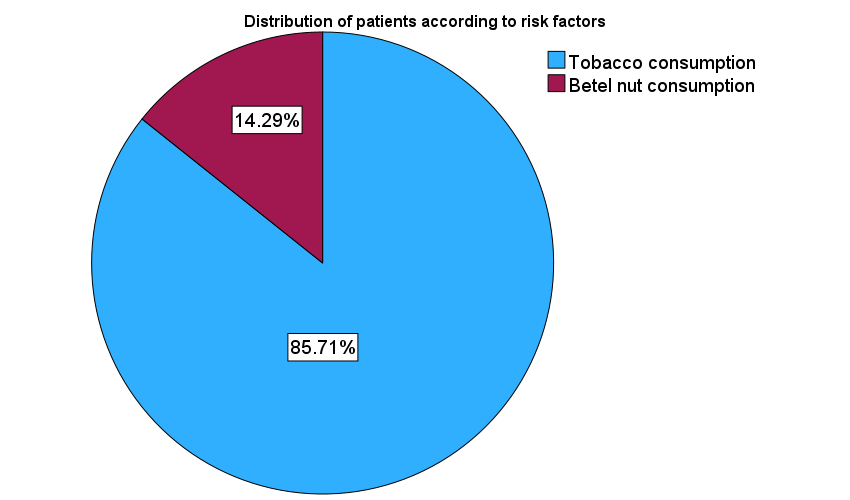
Overall, 73.3% (N=22) of the patients gave a history of smoking or chewing tobacco, while the remaining 26.7 % (N=8) denied tobacco intake. In total-85.7% (N=18) of patients with oral cancer and OPMD confirmed tobacco use and 14.3% (N=3) said that they do not have a habit of tobacco intake but admitted occasional intake of betel nuts. (Fig 4)

Most patients with oral cancer seek treatment in advanced stages, while few seek therapy in earlier stages. In our study, 60% (9/15) of patients with oral cancer presented with stage IV, 20% (3/15) with stage I, 13.3% (2/15) with stage II and 6.7% (1/15) with carcinoma in situ. (Fig 5)

The most common site of oral cancer was the anterior tongue (33.3%, N=5) followed by buccal mucosa (26.7%, N=4), lower gingivobuccal sulcus (20%, N=3) and angle of mouth (20%, N=3). (Fig 6)

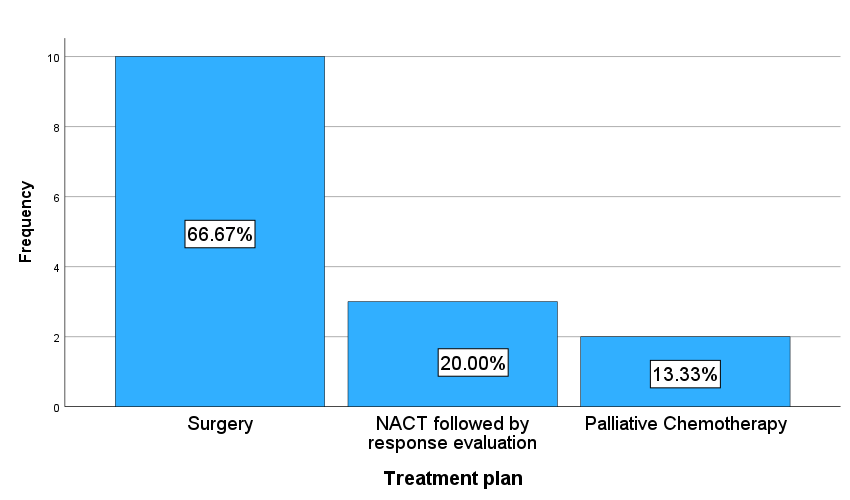
The recommended treatment for patients with oral cancer was surgery in 66.7% (N=10), neo-adjuvant chemotherapy followed by response evaluation in 20% (N=3) and 13.3% (N=2). (Fig 7)

DISCUSSION
This article focuses on the context of setting up a head and neck surgical oncology department in rural Nepal. The common practice of chewing tobacco has made oral cancer a leading cause of cancer-related morbidity and mortality.1–4 Our study also concluded that 85.7% of patients with oral cancer and OPMDs had a history of tobacco intake and placing the chewing form of tobacco products in the lower vestibule of the oral cavity has resulted in buccal mucosa and lower gingivobuccal sulcus to be the commonest site of cancer. The high mortality among oral cancer cases in Nepal is due to late diagnosis in the advanced stage, as there are limited health resources available for early diagnosis of oral cancer.12 The findings also correlate with our study, as 60% of oral cancer patients presented in stage IV. This is particularly due to a lack of awareness in the community resulting in a delay in diagnosis and eventual treatment. Hence, it is important to deliver multimodality treatment in our community for improved survival and outcome of the patients. However, there are numerous challenges in treating head and neck cancer patients in rural areas. Some key issues are: unavailability of infrastructure, lack of specialized doctors, lack of adherence to Multidisciplinary Tumor Boards and protocols, financial constraints, technical limitations, inadequacy in standardization, attitudinal constraints pertinent to behavior, community resistance to change, limitations of the organization and logistics. Our institution has recognized these significant challenges and is trying to overcome these barriers to evolve a smooth process of ‘early detection to treatment’ for cancer cases. Our hospital (BTFCC) is a 25 bedded hospital located in the sub-metropolitan city of Janakpur and has a catchment area of a significantly larger population from the surrounding villages. The hospital possesses basic infrastructure like an operating theatre, Intensive Care Unit (ICU), pathology and histopathology laboratory and departments of surgical oncology, medical oncology, radiology and, emergency with respective specialized doctors, nurses and paramedics in each departments for running a cancer center. The patient is only sent for imaging Computed Tomography/ Magnetic Resonance Imaging and blood bank facility to a nearby (600 m) regional center within the same city. Radiotherapy (RT) availability in a smaller city is a limiting factor, and patients are sent to the nearby neighboring city, approximately 200 km away. However, performing major head and neck surgeries with limited infrastructure is feasible.5,18 Coordination between critical care physicians, nurses and paramedics is necessary with appropriate planning. It is challenging to have facilities like operating theatre with specialized instruments, ICU, imaging, histopathology, blood bank and specialized doctors for cancer treatment in a single institution or even in an entire small town of developing country like Nepal, but our center located in a similar setting possess all basic infrastructure and resources. The setup similar to our hospital is available in most towns in India and has produced satisfactory outcomes.5,18,19 Implementation of a protocol-based treatment is important for attaining improved outcomes. Establishing a multidisciplinary tumor board and adhering to treatment guidelines is the first step in improving outcomes.5 It is often impractical to follow the guidelines of the developed countries in resource- constrained setups and rural communities (like the target population of our study). We have to choose the treatment guidelines based on patient’s preferences that require minimal subsequent intervention with reduced cost and subsequent follow-up but are associated with the maximum efficacy possible. We established a multidisciplinary tumor board with surgical and clinical oncologists and oncology experts from the United States working in this institution. We strictly adhere to treatment guidelines. National Comprehensive Cancer Network (NCCN) guidelines suggest surgery as the preferred treatment of choice for resectable cancer of the oral cavity.20 Surgery includes resection of primary with elective neck dissection.20 Sentinel lymph node is also recently incorporated in guidelines for alternative of neck dissection in selective cases. Still, this option is often not feasible for our patients due to a lack of patient compliance and unaffordability for subsequent intervention and follow-up due to their socio-economic status. The extent of resection, choices of reconstruction, nutrition support and rehabilitation also plays an important role in minimizing postoperative complications.5 As limited resources of the patients plays a vital role in selecting the treatment options, conventional treatment options of radical surgery of primary with elective neck dissection and adjuvant RT is practicable and done in most of our cases. However, this study itself has many limitations because it is not an oncological outcome-based study but lays the foundation for further investigation of the incidence of oral cancer and its associated characteristic trends in different regions across the Madhesh province of Nepal.
CONCLUSION
This article emphasizes the feasibility of delivering multimodality, protocol-based treatment in a resource-constrained set-up. A significant constituent supporting its viability, like appropriate treatment selection, co-ordination and motivation of clinicians, basic infrastructure, and human resources, helps in accomplishing optimal head and neck care in a rural community.
Conflict of Interest
No conflict of interest.
Funding information
N/A.
Ethical statements
The study was conducted after obtaining approval from Institutional Review Board. Being a retrospective study, individual informed consent from subjects were not considered necessary for this study.
Acknowledgement
I would like to address my sincere acknowledgement to Binaytara Foundation Cancer Center for the support provided by them for completing this study.
Author contributions
i. All authors: conception and design
ii. All authors: data collection and assembly
iii. All authors: data analysis, manuscript writing
All authors have approved the manuscript