Purpose of the study
Patients with chronic myeloid leukemia in chronic phase (CML-CP) are treated with tyrosine kinase inhibitors (TKIs) over several years or decades, if not indefinitely. This study aims to evaluate the outcome of patients with CML-CP treated with frontline TKI after a very long-term follow-up of more than 10 years.
Project description
We analyzed patients with newly diagnosed CML-CP and accelerated phase (based solely on the presence of clonal evolution) treated with frontline TKI: standard-dose imatinib, higher-dose imatinib, dasatinib, and nilotinib. The presence of comorbidities was assessed using the Adult Comorbidity Evaluation-27. Patients were evaluated for the achievement of complete cytogenetic response (CCyR), major molecular response (MMR), molecular response with a 4-log reduction (MR4), and molecular response with a 4.5-log reduction (MR4.5). The cumulative incidence of response was assessed with a competing risk model. Event-free survival (EFS), was defined from the date of treatment start to the date of any of the events as defined in the IRIS study, while failure-free survival (FFS) accounted in addition for treatment discontinuation for any reason except of treatment-free remission (TFR). Transformation-free survival (TFS) was defined from the start of therapy to the date of transformation to accelerated or blast phases, and overall survival (OS) to the date of death from any cause or date of last follow-up. We performed univariate and multivariate Cox proportional hazard modelsto evaluate for prognostic factors associated with survival. For variables selection, we used a p-value cutoff of ≤0.10 or less by univariate analysis.
Results and conclusions
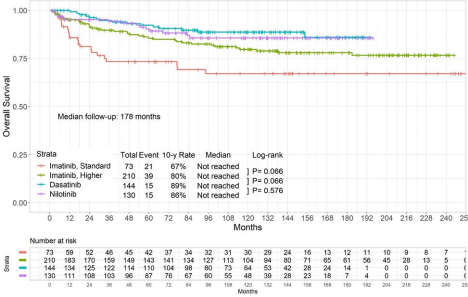
A total of 557 patients were included, with a median age of 49 years (range, 15-86). The overall median follow-up was 178 months (range, 5-254) (standard-dose imatinib, 231 months; higher dose imatinib, 212 months; dasatinib 137 months; nilotinib 138 months) (Table 1). Overall, the 10-year cumulative incidence rates of CCyR, MMR, MR4, and MR4.5 were 91%, 87%, 76%, and 72%, respectively. Patients treated with higher-dose imatinib, dasatinib, and nilotinib had higher cumulative incidence rates of CCyR, MMR, MR4, and MR4.5 compared with standard-dose imatinib. The 10-year FFS rates were 48%, 52%, 67%, and 44% in the standard-dose imatinib, higher-dose imatinib, dasatinib, and nilotinib cohorts, respectively (P<0.001); the 10-year EFS rates were 67%, 80%, 89%, 86%, respectively (P=0.001); and the 10-year OS rates were 67%, 80%, 89%, and 86%, respectively (P=0.206) (Figure 1).

By multivariate analysis, we identified older age, smoking history, higher severity of comorbidities, higher percentage of blasts in peripheral blood, and longer time to achieve CCyR as prognostic factors associated with inferior survival. After a median follow-up of at least 10 years, the 10-year relative survival rate was 91% overall and 94% in patients who achieved CCyR within 1 year of frontline therapy.
In summary, TKI therapy significantly improved the outcome of patients with CML-CP. Treatment with second-generation TKIs in the frontline setting induced higher rates of deep molecular remission than standard-dose imatinib. The choice of frontline TKI did not impact the long-term survival of the patients which was similar to the survival of the general population.